Aflac Cancer and Blood Disorders Center/Children's Healthcare of Atlanta/Emory University, Atlanta, Georgia 30322, USA.
Pediatr Blood Cancer. 2013 Jul;60(7):1141-7. doi: 10.1002/pbc.24398. Epub 2013 Jan 17.
The discovery of effective re-induction regimens for children with more than one relapse of acute lymphoblastic leukemia (ALL) remains elusive. The novel nucleoside analog clofarabine exhibits modest single agent efficacy in relapsed ALL, though optimal combinations of this agent with other active chemotherapy drugs have not yet been defined. Herein we report the response rates of relapsed ALL patients treated on Children's Oncology Group study AAML0523, a Phase I/II study of the combination of clofarabine and cytarabine.
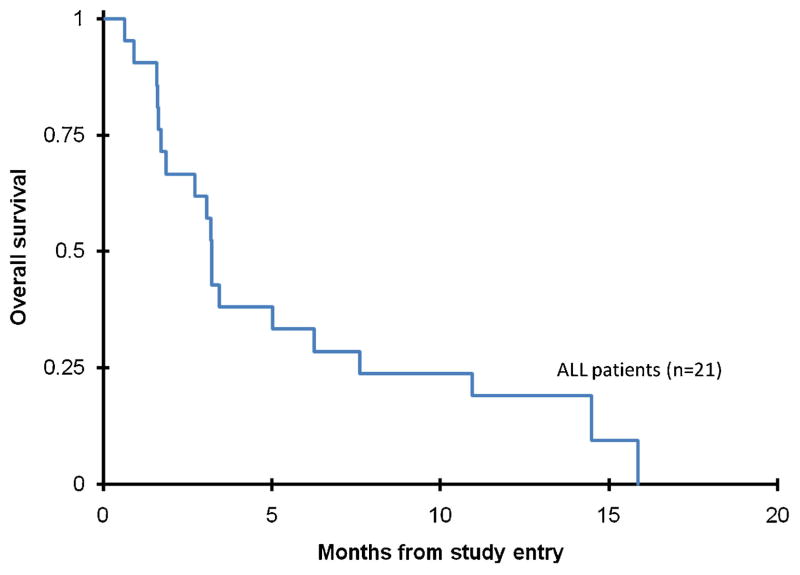
AAML0523 enrolled 21 children with ALL in second or third relapse, or those refractory to re-induction therapy. The study consisted of two phases: a dose finding phase and an efficacy phase. The dose finding portion consisted of a single dose escalation/de-escalation of clofarabine for 5 days in combination with a fixed dose of cytarabine (1 g/m(2)/day for 5 days). Eight patients received clofarabine at 40 mg/m(2)/day and 13 patients at 52 mg/m(2)/day.
Toxicities observed at all doses of clofarabine were typical of intensive chemotherapy regimens for leukemia, with infection being the most common. We did not observe significant hepatotoxicity as reported in other clofarabine combination regimens. The recommended pediatric Phase II dose of clofarabine in combination with cytarabine for the efficacy portion of AAML0523 was 52 mg/m(2). Of 21 patients with ALL, 3 (14%) achieved a complete response (CR). Based on the two-stage design definition of first-stage inactivity, the therapy was deemed ineffective.
The combination of clofarabine and cytarabine in relapsed/refractory childhood ALL does not warrant further clinical investigation.
对于多次复发的急性淋巴细胞白血病(ALL)患儿,仍难以找到有效的再诱导治疗方案。新型核苷类似物克拉屈滨在复发的 ALL 中表现出适度的单药疗效,但尚未确定该药物与其他有效化疗药物的最佳组合。在此,我们报告了在儿童肿瘤学组研究 AAML0523 中接受治疗的复发 ALL 患者的缓解率,该研究为克拉屈滨联合阿糖胞苷的 I/II 期研究。
AAML0523 纳入了 21 例处于第二次或第三次复发的 ALL 患儿,或对再诱导治疗耐药的患儿。该研究分为两个阶段:剂量探索阶段和疗效阶段。剂量探索部分由克拉屈滨联合阿糖胞苷的单剂量递增/递减(连续 5 天,剂量分别为 40 mg/m2/天和 52 mg/m2/天)和固定剂量阿糖胞苷(连续 5 天,剂量为 1 g/m2/天)组成。8 例患儿接受了 40 mg/m2/天的克拉屈滨,13 例患儿接受了 52 mg/m2/天的克拉屈滨。
所有剂量的克拉屈滨均观察到与强化化疗方案相关的毒性反应,感染最为常见。与其他克拉屈滨联合方案报告的情况不同,我们未观察到明显的肝毒性。AAML0523 疗效部分的推荐儿童 II 期剂量为克拉屈滨联合阿糖胞苷 52 mg/m2。21 例 ALL 患儿中,3 例(14%)达到完全缓解(CR)。基于两阶段设计中第一阶段无活性的定义,该治疗被认为无效。
克拉屈滨联合阿糖胞苷治疗复发/难治性儿童 ALL 无效,不值得进一步临床研究。