Norwegian Institute of Public Health, Nydalen, Oslo, Norway.
BMC Infect Dis. 2013 Jan 23;13:30. doi: 10.1186/1471-2334-13-30.
As most genital Chlamydia trachomatis infections are asymptomatic, many patients do not seek health care for testing. Infections remain undiagnosed and untreated. We studied whether screening with information and home sampling resulted in more young people getting tested, diagnosed and treated for chlamydia in the three months following the intervention compared to the current strategy of testing in the health care system.
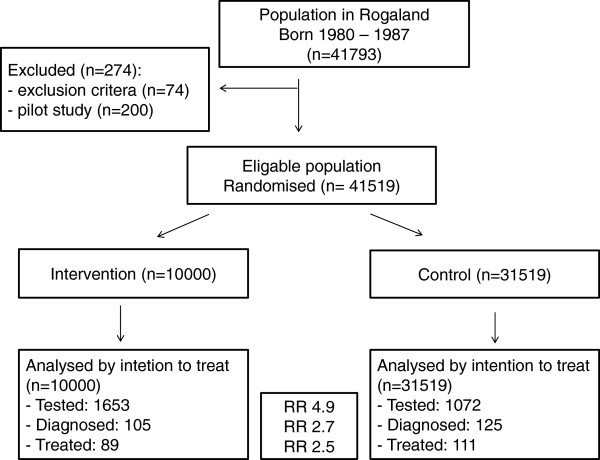
We conducted a population based randomized controlled trial among all persons aged 18-25 years in one Norwegian county (41 519 persons). 10 000 persons (intervention) received an invitation by mail with chlamydia information and a mail-back urine sampling kit. 31 519 persons received no intervention and continued with usual care (control). All samples from both groups were analysed in the same laboratory. Information on treatment was obtained from the Norwegian Prescription Database (NorPD). We estimated risk ratios and risk differences of being tested, diagnosed and treated in the intervention group compared to the control group.
In the intervention group 16.5% got tested and in the control group 3.4%, risk ratio 4.9 (95% CI 4.5-5.2). The intervention led to 2.6 (95% CI 2.0-3.4) times as many individuals being diagnosed and 2.5 (95% CI 1.9-3.4) times as many individuals receiving treatment for chlamydia compared to no intervention in the three months following the intervention.
In Norway, systematic screening with information and home sampling results in more young people being tested, diagnosed and treated for chlamydia in the three months following the intervention than the current strategy of testing in the health care system. However, the study has not established that the intervention will reduce the chlamydia prevalence or the risk of complications from chlamydia.
由于大多数生殖器沙眼衣原体感染无症状,许多患者不会因检测而寻求医疗保健。感染仍然未被诊断和未被治疗。我们研究了通过信息和家庭采样进行筛查是否会导致更多的年轻人在干预后三个月内接受衣原体检测、诊断和治疗,与目前在医疗保健系统中进行检测的策略相比。
我们在挪威一个县的所有 18-25 岁人群中进行了一项基于人群的随机对照试验(41519 人)。10000 人(干预组)收到了一封带有衣原体信息和邮寄尿液采样试剂盒的邮件邀请。31519 人未接受干预,继续接受常规护理(对照组)。两组的所有样本均在同一实验室进行分析。治疗信息来自挪威处方数据库(NorPD)。我们估计了干预组与对照组在检测、诊断和治疗方面的风险比和风险差异。
干预组有 16.5%的人接受了检测,而对照组只有 3.4%,风险比为 4.9(95%CI 4.5-5.2)。干预措施导致诊断的人数增加了 2.6 倍(95%CI 2.0-3.4),接受衣原体治疗的人数增加了 2.5 倍(95%CI 1.9-3.4),与干预后三个月内没有干预相比。
在挪威,系统的筛查与信息和家庭采样相结合,可使更多的年轻人在干预后三个月内接受衣原体检测、诊断和治疗,而不是目前在医疗保健系统中进行检测的策略。然而,该研究并未证实干预措施会降低衣原体流行率或衣原体感染并发症的风险。