AP-HP, Jean Verdier Hospital, Paris 13 University, Sorbonne Paris Cité, Department of Endocrinology, Diabetology, and Nutrition, CRNH-IdF, Bondy, France.
Diabetes Care. 2013 Jul;36(7):2070-6. doi: 10.2337/dc12-1780. Epub 2013 Feb 1.
We investigated whether glycation gap (G-Gap), an index of intracellular glycation of proteins, was associated with diabetes complications.
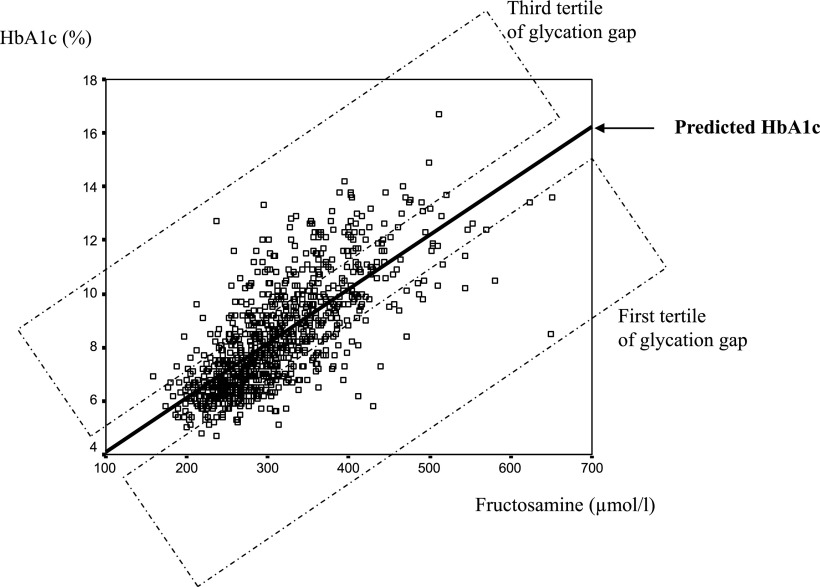
We measured concomitantly HbA1c and fructosamine in 925 patients with type 2 diabetes to calculate the G-Gap, defined as the difference between measured HbA1c, and fructosamine-based predicted HbA1c. Patients were explored for retinopathy, nephropathy, peripheral neuropathy, cardiac autonomic neuropathy (n = 512), and silent myocardial ischemia (n = 506).
Macroproteinuria was the only complication that was associated with G-Gap (prevalence in the first, second, and third tertile of G-Gap: 2.9, 6.2, and 11.0%, respectively; P < 0.001). The G-Gap was higher in patients with macroproteinuria than in those without (1.06 ± 1.62 vs. 0.03 ± 1.30%; P < 0.0001). Because HbA1c was associated with both G-Gap (HbA1c 7.0 ± 1.4, 7.9 ± 1.4, and 10.1 ± 1.8% in the first, second, and third G-Gap tertile, respectively; P < 0.0001) and macroproteinuria (HbA1c 8.8 ± 2.2% if macroproteinuria, 8.3 ± 2.0% if none; P < 0.05), and because it could have been a confounder, we matched 54 patients with macroproteinuria and 200 patients without for HbA1c. Because macroproteinuria was associated with lower serum albumin and fructosamine levels, which might account for higher G-Gap, we calculated in this subpopulation albumin-indexed fructosamine and G-Gap; macroproteinuria was independently associated with male sex (odds ratio [OR] 3.2 [95% CI 1.5-6.7]; P < 0.01), hypertension (2.9 [1.1-7.5]; P < 0.05), and the third tertile of albumin-indexed G-Gap (2.3 [1.1-4.4]; P < 0.05) in multivariate analysis.
In type 2 diabetic patients, G-Gap was associated with macroproteinuria, independently of HbA1c, albumin levels, and confounding factors, suggesting a specific role of intracellular glycation susceptibility on kidney glomerular changes.
我们旨在研究糖基化间隙(G-Gap),一种衡量蛋白质细胞内糖化的指标,是否与糖尿病并发症相关。
我们同时测量了 925 名 2 型糖尿病患者的糖化血红蛋白(HbA1c)和果糖胺,以计算 G-Gap,定义为测量的 HbA1c 与基于果糖胺预测的 HbA1c 之间的差值。在这些患者中探索了视网膜病变、肾病、周围神经病变、心脏自主神经病变(n=512)和无症状性心肌缺血(n=506)。
大量蛋白尿是唯一与 G-Gap 相关的并发症(G-Gap 第一、二、三分位组的患病率分别为 2.9%、6.2%和 11.0%;P<0.001)。大量蛋白尿患者的 G-Gap 高于无大量蛋白尿患者(1.06±1.62 比 0.03±1.30%;P<0.0001)。因为 HbA1c 与 G-Gap 相关(HbA1c 分别为 7.0±1.4、7.9±1.4 和 10.1±1.8%,在 G-Gap 的第一、二、三分位组中;P<0.0001)和大量蛋白尿相关(如果有大量蛋白尿,则 HbA1c 为 8.8±2.2%;如果没有,则 HbA1c 为 8.3±2.0%;P<0.05),并且可能是一个混杂因素,我们将 54 名大量蛋白尿患者和 200 名无大量蛋白尿患者按照 HbA1c 进行匹配。由于大量蛋白尿与较低的血清白蛋白和果糖胺水平相关,这可能导致 G-Gap 升高,因此我们在这个亚群中计算了白蛋白校正的果糖胺和 G-Gap;大量蛋白尿与男性(比值比[OR]3.2[95%置信区间 1.5-6.7];P<0.01)、高血压(2.9[1.1-7.5];P<0.05)和白蛋白校正的 G-Gap 三分位组(2.3[1.1-4.4];P<0.05)独立相关。
在 2 型糖尿病患者中,G-Gap 与大量蛋白尿相关,独立于 HbA1c、白蛋白水平和混杂因素,提示细胞内糖化易感性对肾小球变化有特定作用。