Division of Clinical Pharmacology, University of Cape Town, Cape Town, South Africa.
PLoS One. 2013;8(2):e53570. doi: 10.1371/journal.pone.0053570. Epub 2013 Feb 6.
Providing private antiretroviral therapy (ART) care for public sector patients could increase access to ART in low- and middle-income countries. We compared the costs and outcomes of a private-care and a public-care ART program in South Africa.
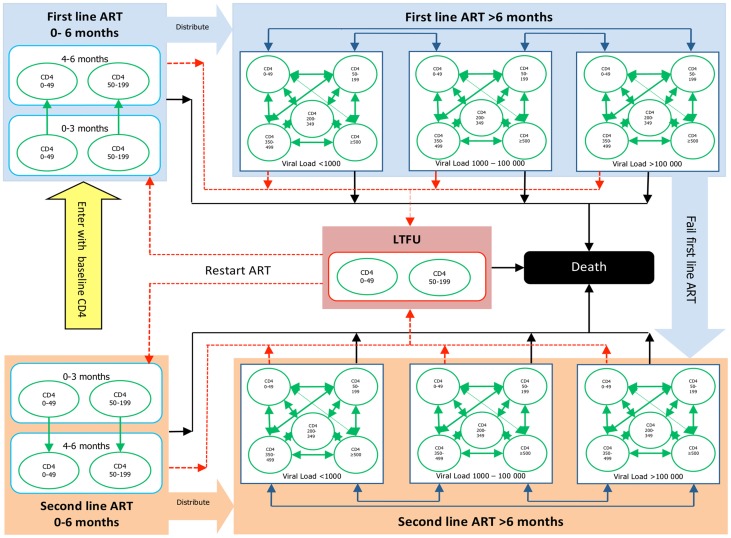
A novel Markov model was developed from the public-care program. Patients were first tunneled for 6 months in their baseline CD4 category before being distributed into a dynamic CD4 and viral load model. Patients were allowed to return to ART care from loss to follow up (LTFU). We then populated this modeling framework with estimates derived from the private-care program to externally validate the model.
Baseline characteristics were similar in the two programs. Clinic visit utilization was higher and death rates were lower in the first few years on ART in the public-care program. After 10 years on ART we estimated the following outcomes in the public-care and private-care programs respectively: viral load <1000 copies/ml 89% and 84%, CD4 >500 cells/μl 33% and 37%, LTFU 14% and 14%, and death 27% and 32%. Lifetime undiscounted survival estimates were 14.1 (95%CI 13.2-14.9) and (95%CI 12.7-14.5) years with costs of 18,734 (95%CI 12,588-14,022) and 13,062 (95%CI 12,077-14,047) USD in the private-care and public-care programs respectively. When clinic visit utilization in the public-care program was reduced by two thirds after the initial 6 months on ART, which is similar to their current practice, the costs were comparable between the programs.
Using a novel Markov model, we determined that the private-care program had similar outcomes but lower costs than the public-care program, largely due to lower visit frequencies. These findings have important implications for increasing and sustaining coverage of patients in need of ART care in resource-limited settings.
为公共部门的患者提供私人抗逆转录病毒治疗(ART)服务可以增加中低收入国家获得 ART 的机会。我们比较了南非私人护理和公共护理 ART 项目的成本和结果。
从公共护理项目中开发了一种新的马尔可夫模型。患者在基线 CD4 类别中首先接受 6 个月的隧道治疗,然后被分配到一个动态 CD4 和病毒载量模型中。允许患者从失访(LTFU)返回 ART 护理。然后,我们使用私人护理计划中的估计值填充这个建模框架,以对外验证模型。
两个项目的基线特征相似。在公共护理计划的最初几年,ART 治疗期间的就诊利用率更高,死亡率更低。在接受 ART 治疗 10 年后,我们分别估计了公共护理和私人护理计划的以下结果:病毒载量<1000 拷贝/ml 分别为 89%和 84%,CD4>500 个细胞/μl 分别为 33%和 37%,LTFU 分别为 14%和 14%,死亡分别为 27%和 32%。终生未贴现生存率估计分别为 14.1(95%CI 13.2-14.9)和 12.7-14.5)年,私人护理和公共护理计划的成本分别为 18734(95%CI 12588-14022)和 13062(95%CI 12077-14047)美元。当公共护理计划在接受 ART 治疗后的最初 6 个月后将就诊利用率减少三分之二时,这与他们目前的做法相似,两个计划的成本相当。
使用新的马尔可夫模型,我们确定私人护理计划的结果与公共护理计划相似,但成本较低,这主要是由于就诊频率较低。这些发现对在资源有限的环境中增加和维持需要 ART 护理的患者的覆盖范围具有重要意义。