Ministry of Health and Family Welfare, Government of India, New Delhi, India.
Glob Health Action. 2013 Mar 1;6:1-11. doi: 10.3402/gha.v6i0.20135.
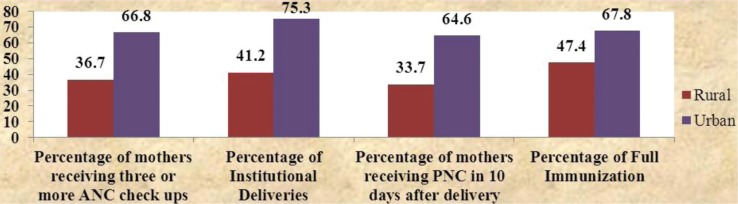
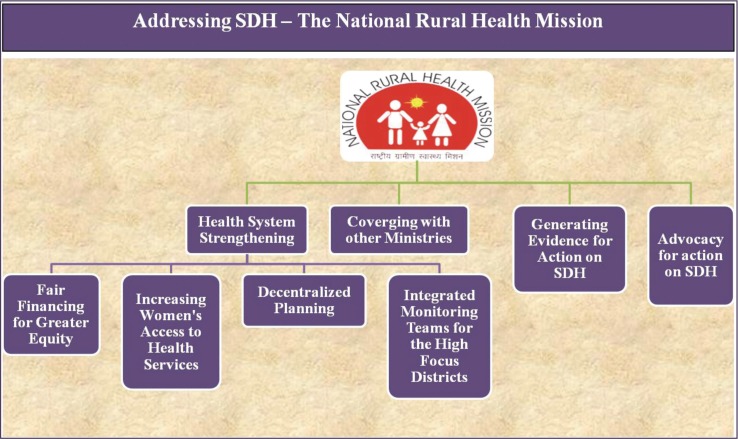
At the turn of the 21st century, India was plagued by significant rural-urban, inter-state and inter-district inequities in health. For example, in 2004, the infant mortality rate (IMR) was 24 points higher in rural areas compared to urban areas. To address these inequities, to strengthen the rural health system (a major determinant of health in itself) and to facilitate action on other determinants of health, India launched the National Rural Health Mission (NRHM) in April 2005.
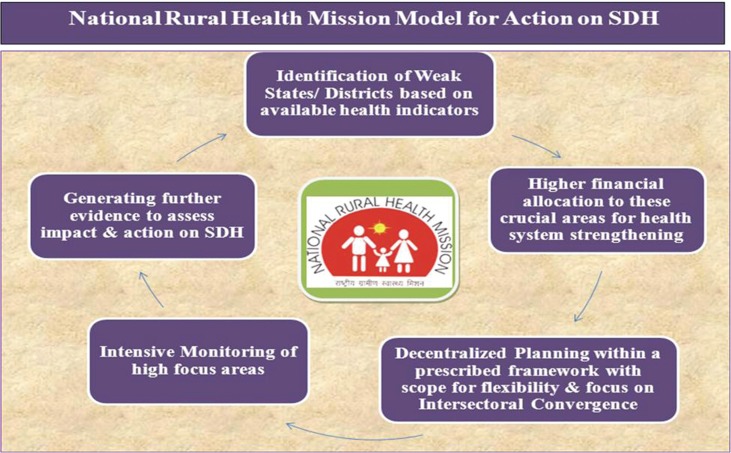
Under the NRHM, Rs. 666 billion (US$12.1 billion) was invested in rural areas from April 2005 to March 2012. There was also a substantially higher allocation for 18 high-focus states and 264 high-focus districts, identified on the basis of poor health and demographic indicators. Other determinants of health, especially nutrition and decentralized action, were addressed through mechanisms like State/District Health Missions, Village Health, Sanitation and Nutrition Committees, and Village Health and Nutrition Days.
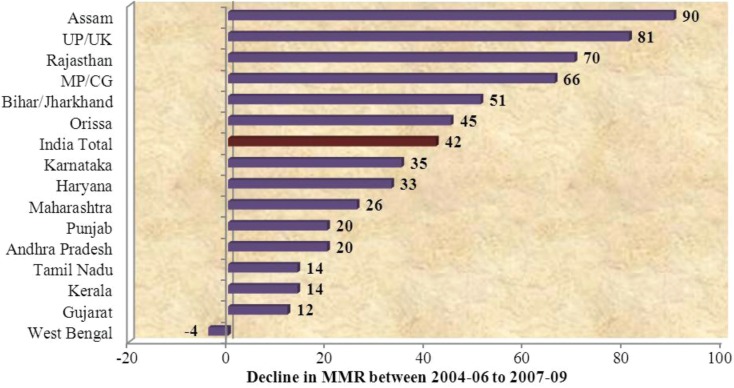
Consequently, in bigger high-focus states, rural IMR fell by 15.6 points between 2004 and 2011, as compared to 9 points in urban areas. Similarly, the maternal mortality rate in high-focus states declined by 17.9% between 2004-2006 and 2007-2009 compared to 14.6% in other states.
The article, on the basis of the above approaches employed under NRHM, proposes the NRHM model to 'reduce health inequities and initiate action on SDH'.
在 21 世纪之交,印度在城乡、州际和地区间的卫生方面存在着显著的不平等。例如,2004 年,农村地区的婴儿死亡率(IMR)比城市地区高 24 个百分点。为了解决这些不平等问题,加强农村卫生系统(本身是健康的主要决定因素),并促进对其他健康决定因素的行动,印度于 2005 年 4 月启动了国家农村卫生使命(NRHM)。
在 NRHM 下,从 2005 年 4 月到 2012 年 3 月,在农村地区投资了 6660 亿卢比(121 亿美元)。在根据卫生和人口指标较差而确定的 18 个重点州和 264 个重点区,也有大幅增加的拨款。其他健康决定因素,特别是营养和权力下放行动,是通过州/地区卫生使命、农村卫生、环境卫生和营养委员会以及农村卫生和营养日等机制来解决的。
因此,在较大的重点州,农村 IMR 在 2004 年至 2011 年期间下降了 15.6 个百分点,而城市地区则下降了 9 个百分点。同样,重点州的产妇死亡率在 2004-2006 年至 2007-2009 年期间下降了 17.9%,而其他州则下降了 14.6%。
本文根据 NRHM 下采用的上述方法,提出了 NRHM 模式,以“减少卫生不平等,启动对 SDH 的行动”。