May Taymaa, Shoni Melina, Vitonis Allison F, Quick Charles M, Growdon Whitfield B, Muto Michael G
Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA 02115, USA ; Division of Gynecologic Oncology, Dana-Farber Cancer Institute, Boston, MA 02115, USA.
Int J Surg Oncol. 2013;2013:858916. doi: 10.1155/2013/858916. Epub 2013 Feb 27.
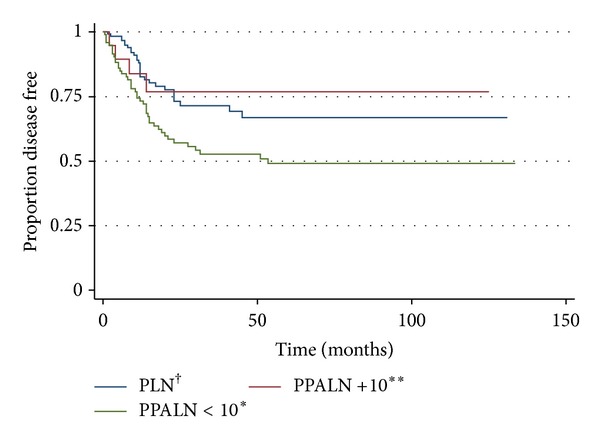
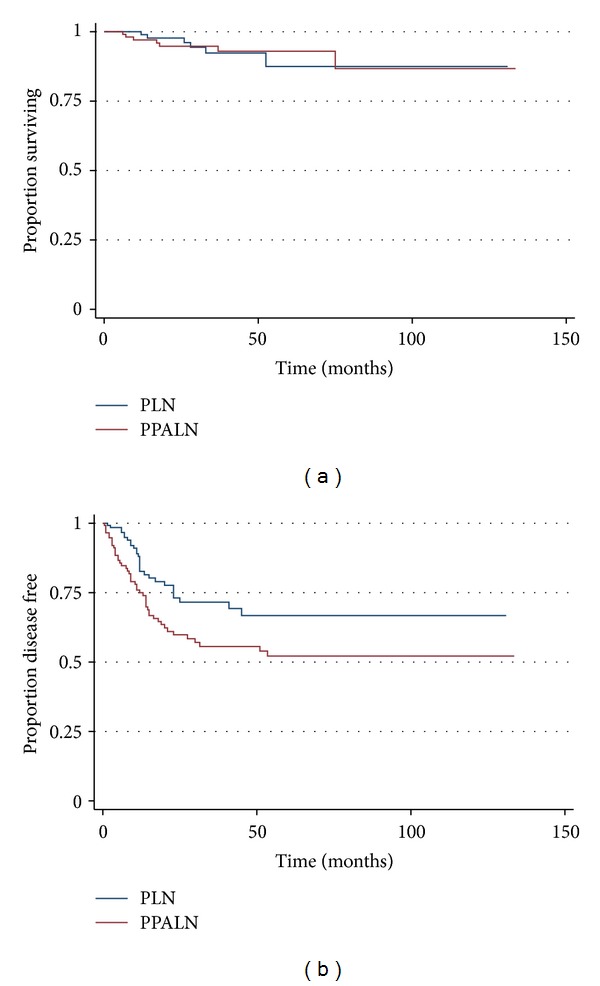
Objectives. To characterize clinical outcomes in patients with intermediate or high-risk endometrial carcinoma who underwent surgical staging with or without para-aortic lymphadenectomy. Methods. This is a retrospective cohort study of patients with intermediate or high-risk endometrial adenocarcinoma who underwent surgical staging with (PPALN group) or without (PLN) para-aortic lymphadenectomy. Data were collected, Kaplan-Meier curves were generated, and univariate and multivariate analyses performed to compare differences in adjuvant therapy, disease recurrence, disease-free survival (DFS), and overall survival (OS). Results. 118 patients were included in the PPALN group and 139 in the PLN group. Patients in the PPALN group were more likely to receive adjuvant vaginal brachytherapy (25.4% versus 11.5%, OR = 2.5, P = 0.03) and less likely to receive adjuvant multimodal combination therapy (17.81% versus 28.8%, OR = 0.28, P = 0.002). DFS was improved in the PLN group as compared to PPALN (80% versus 62%, P = 0.02). OS was equivalent (P = 0.93). Patients in the PPALN group who had less than 10 para-aortic nodes removed were twice as likely to recur than patients who had 10 or more para-aortic nodes or patients in the PLN group (HR 2.08, CI 1.20-3.60, P = 0.009). Conclusions. Patients in the PLN group were more likely to receive multimodal adjuvant therapy and had better DFS than the PPALN group. Pelvic lymphadenectomy followed by adjuvant radiation and chemotherapy may represent an effective treatment option for patients with intermediate or high-risk disease. If systematic para-aortic lymphadenectomy is performed and less than 10 para-aortic lymph nodes are obtained, multimodality adjuvant therapy should be considered to improve DFS.
目的。对接受或未接受主动脉旁淋巴结清扫术进行手术分期的中高危子宫内膜癌患者的临床结局进行特征描述。方法。这是一项对接受或未接受主动脉旁淋巴结清扫术(PPALN组)进行手术分期的中高危子宫内膜腺癌患者的回顾性队列研究。收集数据,绘制Kaplan-Meier曲线,并进行单因素和多因素分析,以比较辅助治疗、疾病复发、无病生存期(DFS)和总生存期(OS)的差异。结果。PPALN组纳入118例患者,PLN组纳入139例患者。PPALN组患者更有可能接受辅助阴道近距离放疗(25.4%对11.5%,OR = 2.5,P = 0.03),而接受辅助多模式联合治疗的可能性较小(17.81%对28.8%,OR = 0.28,P = 0.002)。与PPALN组相比,PLN组的DFS有所改善(80%对62%,P = 0.02)。OS相当(P = 0.93)。PPALN组中切除少于10个主动脉旁淋巴结的患者复发的可能性是切除10个或更多主动脉旁淋巴结的患者或PLN组患者的两倍(HR 2.08,CI 1.20 - 3.60,P = 0.009)。结论。PLN组患者比PPALN组更有可能接受多模式辅助治疗,且DFS更好。盆腔淋巴结清扫术联合辅助放疗和化疗可能是中高危疾病患者的一种有效治疗选择。如果进行系统性主动脉旁淋巴结清扫术且获得的主动脉旁淋巴结少于10个,则应考虑多模式辅助治疗以改善DFS。