Toptas Tayfun, Simsek Tayup
Department of Obstetrics and Gynaecology, Division of Gynaecologic Oncological Surgery, Akdeniz University Hospital, Antalya, Konyaaltı 07070, Turkey.
Oncol Lett. 2015 Jan;9(1):355-364. doi: 10.3892/ol.2014.2653. Epub 2014 Oct 31.
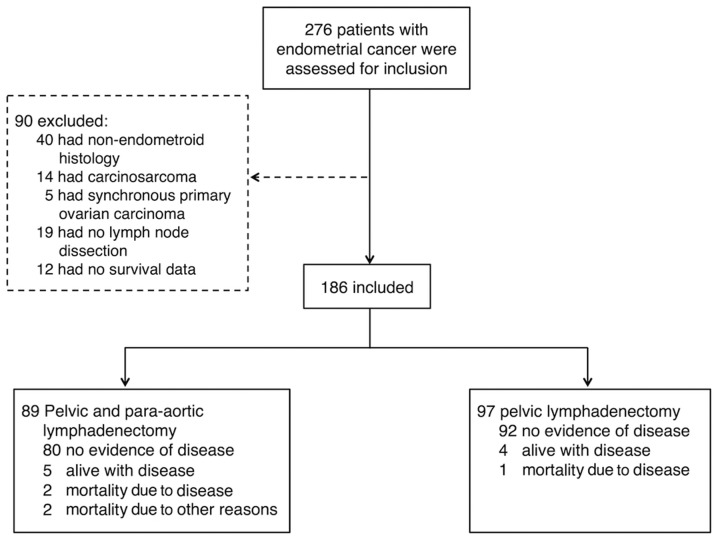
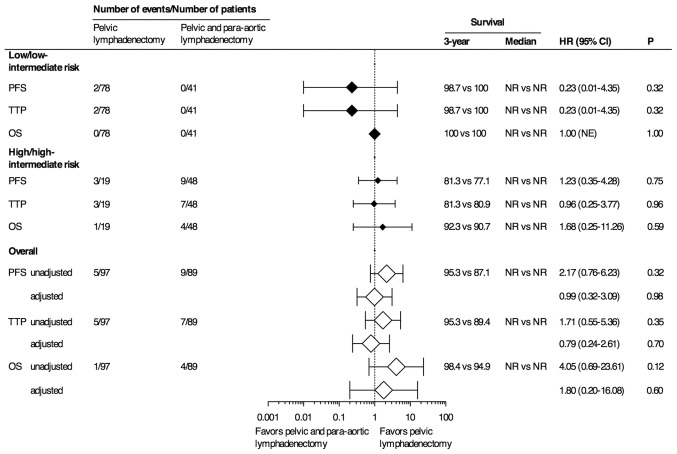
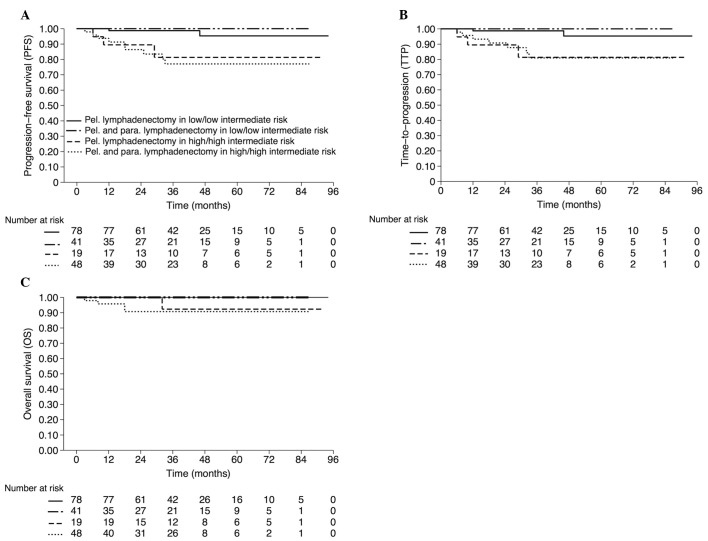
The therapeutic benefit of lymphadenectomy in patients exhibiting endometrial cancer (EC) remains controversial. The aim of the present study was to determine whether the addition of para-aortic lymphadenectomy to pelvic lymphadenectomy (PLND) improves survival in patients with endometrioid type EC. A single tertiary-center, retrospective analysis was conducted in a total of 186 patients who were surgically treated with either PLND alone (n=97) or combined pelvic and para-aortic lymphadenectomy (PPaLND; n=89). Adjuvant treatments were assigned according to the Gynecologic Oncology Group (GOG) risk of recurrence analysis. The primary endpoint of the present study was progression-free survival (PFS). The median follow-up time was 38 months (95% confidence interval, 36.47-42.90) for all patients. No statistically significant differences were identified between the two groups in terms of overall survival (OS), PFS or time to progression (TTP). Kaplan-Meier estimates of three-year OS, PFS and TTP for patients with low or low-intermediate risk were as follows: PLND, 100, 98.7 and 98.7%, respectively; and PPaLND, all 100%. The estimated three-year OS, PFS and TTP for patients with high or high-intermediate risk were as follows: PLND, 92.3, 81.3 and 81.3%; and PPaLND, 90.7, 77.1 and 80.9%, respectively. No statistically significant differences were detected in the three-year OS, PFS and TTP between the lymphadenectomy groups, regardless of the GOG risk of recurrence (PLND, 98.4, 95.3 and 95.3%; and PPaLND, 94.9, 87.1 and 89.4%). Therefore, the combination treatment, PPaLND did not provide any survival advantage over pelvic lymphadenectomy alone.
对于子宫内膜癌(EC)患者,淋巴结切除术的治疗益处仍存在争议。本研究的目的是确定在盆腔淋巴结切除术(PLND)基础上加行腹主动脉旁淋巴结切除术是否能提高子宫内膜样型EC患者的生存率。对总共186例接受单纯PLND(n = 97)或盆腔及腹主动脉旁淋巴结联合切除术(PPaLND;n = 89)手术治疗的患者进行了单中心回顾性分析。辅助治疗根据妇科肿瘤学组(GOG)复发风险分析进行分配。本研究的主要终点是无进展生存期(PFS)。所有患者的中位随访时间为38个月(95%置信区间,36.47 - 42.90)。两组在总生存期(OS)、PFS或疾病进展时间(TTP)方面未发现统计学上的显著差异。低风险或低中风险患者的三年OS、PFS和TTP的Kaplan-Meier估计值如下:PLND组分别为100%、98.7%和98.7%;PPaLND组均为100%。高风险或高中风险患者患者患者的三年OS、PFS和TTP估计值如下:PLND组分别为92.3%、81.3%和81.3%;PPaLND组分别为90.7%、77.1%和80.9%。无论GOG复发风险如何,淋巴结切除术组之间的三年OS、PFS和TTP均未检测到统计学上的显著差异(PLND组分别为98.4%、95.3%和95.3%;PPaLND组分别为94.9%、87.1%和89.4%)。因此,联合治疗PPaLND相对于单纯盆腔淋巴结切除术并未提供任何生存优势。