Koene Bart M, Soliman Hamad Mohamed A, Bouma Wobbe, Mariani Massimo A, Peels Kathinka C, van Dantzig Jan-Melle, van Straten Albert H
J Cardiothorac Surg. 2013 Apr 17;8:96. doi: 10.1186/1749-8090-8-96.
The influence of prosthesis-patient mismatch (PPM) on survival after aortic valve replacement (AVR) remains controversial. In this study, we sought to determine the effect of PPM on early (≤30 days) and late mortality (>30 days) after AVR or AVR combined with coronary artery bypass grafting (AVR with CABG).
Between January 1998 and March 2012, 2976 patients underwent AVR (n= 1718) or AVR with CABG (n=1258) at a single institution. PPM was defined as an indexed effective orifice area (EOAI) ≤0.85 cm2/m2 and patients were divided into two groups based on the existence of PPM. Cumulative probability values of survival were estimated with Kaplan-Meier method and compared between groups using Breslow test. Univariate and multivariate independent predictors of early mortality were identified using logistic regression. Cox proportional-hazard regression analysis was used to determine univariate and multivariate independent predictors of late mortality.
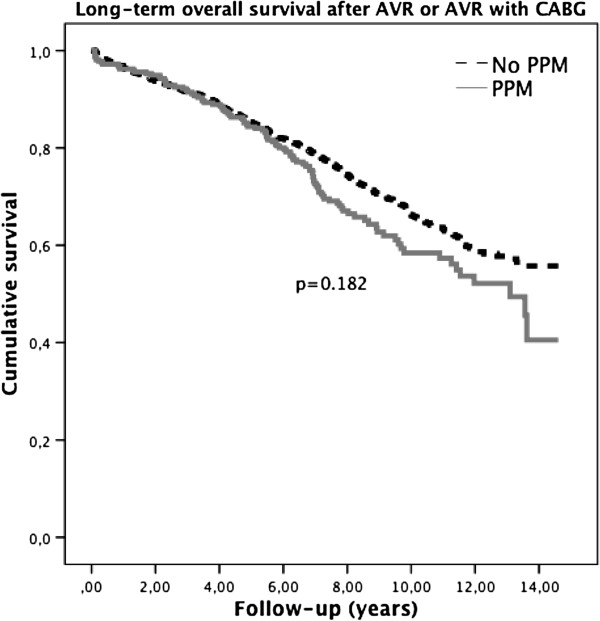
Early mortality was 6.7% in the PPM group vs 4.7% in the group with no PPM (p=0.013). Late mortality for the PPM group at 1, 5 and 10 years was 4%, 16% and 43%, respectively. Late mortality for the group with no PPM at 1, 5 and 10 years was 4%, 15% and 33% respectively. Independent predictors of early mortality included age, severely impaired left ventricular (LV) function, endocarditis, renal dysfunction, chronic obstructive pulmonary disease (COPD) and cardiopulmonary bypass (CPB) time. Multivariate independent predictors of late mortality included age, severely impaired LV function, diabetes, peripheral vascular disease (PVD), renal dysfunction, history of a cerebrovascular accident (CVA), CPB time and a history of previous cardiac surgery. PPM was not an independent predictor of early or late mortality.
PPM is not an independent predictor of both early and late mortality after AVR or AVR combined with CABG.
人工瓣膜-患者不匹配(PPM)对主动脉瓣置换术(AVR)后生存率的影响仍存在争议。在本研究中,我们试图确定PPM对AVR或AVR联合冠状动脉旁路移植术(AVR合并CABG)后早期(≤30天)和晚期死亡率(>30天)的影响。
1998年1月至2012年3月期间,2976例患者在单一机构接受了AVR(n = 1718)或AVR合并CABG(n = 1258)。PPM定义为指数化有效瓣口面积(EOAI)≤0.85 cm2/m2,患者根据是否存在PPM分为两组。采用Kaplan-Meier法估计生存累积概率值,并使用Breslow检验在组间进行比较。使用逻辑回归确定早期死亡率的单因素和多因素独立预测因素。采用Cox比例风险回归分析确定晚期死亡率的单因素和多因素独立预测因素。
PPM组早期死亡率为6.7%,无PPM组为4.7%(p = 0.013)。PPM组1年、5年和10年的晚期死亡率分别为4%、16%和43%。无PPM组1年、5年和10年的晚期死亡率分别为4%、15%和33%。早期死亡率的独立预测因素包括年龄、左心室(LV)功能严重受损、心内膜炎、肾功能不全、慢性阻塞性肺疾病(COPD)和体外循环(CPB)时间。晚期死亡率的多因素独立预测因素包括年龄、LV功能严重受损、糖尿病、外周血管疾病(PVD)、肾功能不全、脑血管意外(CVA)病史、CPB时间和既往心脏手术史。PPM不是早期或晚期死亡率的独立预测因素。
PPM不是AVR或AVR联合CABG后早期和晚期死亡率的独立预测因素。