Medicine Service, Birmingham VA Medical Center and Department of Medicine, University of Alabama at Birmingham, Birmingham, Alabama, USA.
BMJ Open. 2013 Apr 18;3(4). doi: 10.1136/bmjopen-2012-002157. Print 2013.
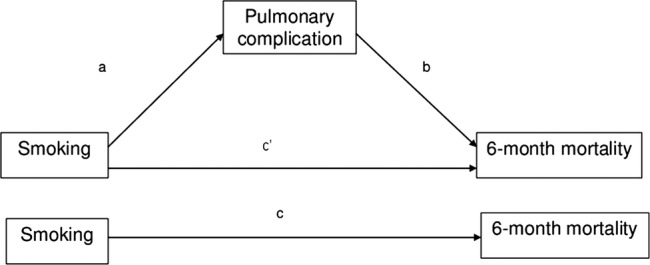
To assess the mediation of smoking-associated postoperative mortality by postoperative complications.
Observational cohort study.
Using data from the Veterans Affairs (VA) Surgical Quality Improvement Programme, a quality assurance programme for major surgical procedures in the VA healthcare system, we assessed the association of current smoking at the time of the surgery with 6-month and 1-year mortality.
Using mediation analyses, we calculated the relative contribution of each smoking-associated complication to smoking-associated postoperative mortality, both unadjusted and adjusted for age, race/ethnicity, work relative value unit of the operation, surgeon specialty, American Society of Anesthesiologists class and year of surgery. Smoking-associated complications included surgical site infection (SSI), cardiovascular complications (myocardial infarction, cardiac arrest and/or stroke) and pulmonary complications (pneumonia, failure to wean and/or reintubation).
There were 186 632 never smokers and 135 741 current smokers. The association of smoking and mortality was mediated by smoking-related complications with varying effects. In unadjusted analyses, the proportions of mediation of smoking to 6-month mortality explained by the complications were as follows: SSIs 22%, cardiovascular complications 12% and pulmonary complications 89%. In adjusted analyses, the per cents mediated by each complication were as follows: SSIs 2%, cardiovascular complications 4% and pulmonary complications 22%. In adjusted analyses for 1-year mortality, respective per cents mediated were 2%, 3% and 16%.
Pulmonary complications, followed by cardiovascular complications and SSIs were mediators of smoking-associated 6-month and 1-year mortality. Interventions targeting smoking cessation and prevention and early treatment of pulmonary complications has the likelihood of reducing postoperative mortality after elective surgery.
评估吸烟相关术后并发症对术后死亡率的中介作用。
观察性队列研究。
利用退伍军人事务部(VA)手术质量改进计划的数据,该计划是 VA 医疗保健系统中主要手术的质量保证计划,我们评估了手术时吸烟与 6 个月和 1 年死亡率的相关性。
使用中介分析,我们计算了每种与吸烟相关的并发症对与吸烟相关的术后死亡率的相对贡献,既未调整也未调整年龄、种族/族裔、手术的工作相对价值单位、外科医生专业、美国麻醉师协会分类和手术年份。与吸烟相关的并发症包括手术部位感染(SSI)、心血管并发症(心肌梗死、心脏骤停和/或中风)和肺部并发症(肺炎、脱机失败和/或重新插管)。
有 186632 名从不吸烟者和 135741 名当前吸烟者。吸烟与死亡率的关联是由与吸烟相关的并发症介导的,其影响程度不同。在未调整的分析中,并发症对 6 个月死亡率的中介作用比例如下:SSI 22%、心血管并发症 12%和肺部并发症 89%。在调整分析中,每种并发症的中介百分比如下:SSI 2%、心血管并发症 4%和肺部并发症 22%。在调整后的 1 年死亡率分析中,分别为 2%、3%和 16%。
肺部并发症、心血管并发症和 SSI 是吸烟相关 6 个月和 1 年死亡率的中介。针对戒烟和预防以及早期治疗肺部并发症的干预措施有可能降低择期手术后的死亡率。