KFH Nierenzentrum Muenchen-Laim, Elsenheimerstr 36, 80687 Munich, Germany.
BMC Nephrol. 2013 Apr 23;14:93. doi: 10.1186/1471-2369-14-93.
Nasal colonization with methicillin-resistant Staphylococcus aureus (MRSA) is a well defined risk factor for subsequent bacteremia and death in various groups of patients, but its impact on outcome in patients receiving long-term hemodialysis (HD) is under debate.
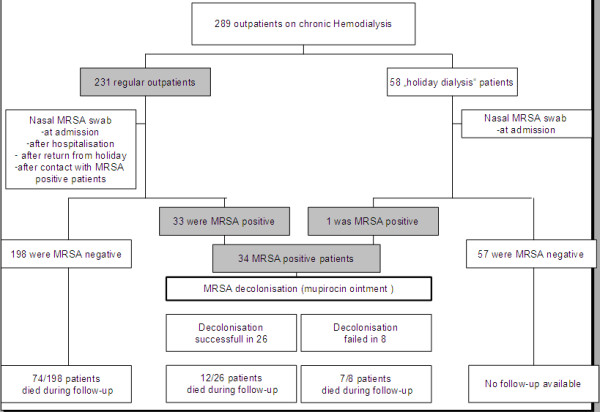
This prospective interventional cohort study (performed 2004 to 2010) enrolled 289 HD outpatients of an urban dialysis-unit. Nasal swab cultures for MRSA were performed in all patients upon first admission, at transfer from another dialysis facility or readmission after hospitalisation. Nasal MRSA carriers were treated in a separate ward and received mupirocin nasal ointment. Concomitant extra-nasal MRSA colonization was treated with 0.2% chlorhexidine mouth rinse (throat) or octenidine dihydrochloride containing antiseptic soaps and 2% chlorhexidine body washes (skin). Clinical data and outcome of carriers and noncarriers were systematically analyzed.
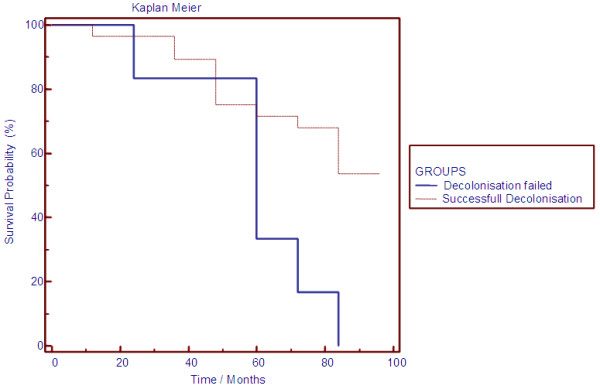
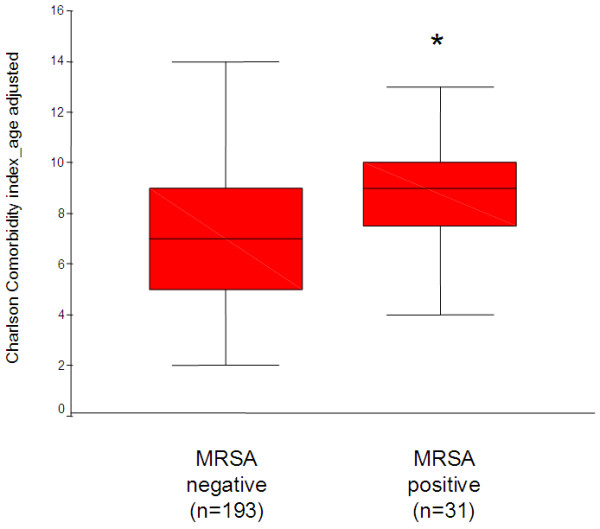
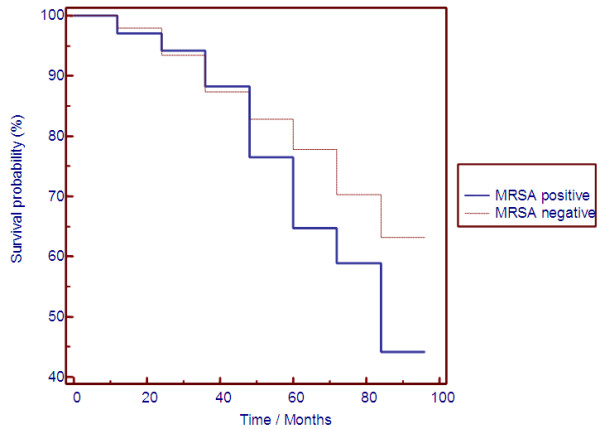
The screening approach identified 34 nasal MRSA carriers (11.7%). Extra-nasal MRSA colonization was observed in 11/34 (32%) nasal MRSA carriers. History of malignancy and an increased Charlson Comorbidity Index were significant predictors for nasal MRSA carriers, whereas traditional risk factors for MRSA colonization or markers of inflammation or malnutrition were not able to discriminate. Kaplan-Meier analysis demonstrated significant survival differences between MRSA carriers and noncarriers. Mupirocin ointment persistently eliminated nasal MRSA colonization in 26/34 (73.5%) patients. Persistent nasal MRSA carriers with failure of this eradication approach had an extremely poor prognosis with an all-cause mortality rate >85%.
Nasal MRSA carriage with failure of mupirocin decolonization was associated with increased mortality despite a lack of overt clinical signs of infection. Further studies are needed to demonstrate whether nasal MRSA colonization represents a novel predictor of worse outcome or just another surrogate marker of the burden of comorbid diseases leading to fatal outcome in HD patients.
耐甲氧西林金黄色葡萄球菌(MRSA)鼻腔定植是各种患者发生随后菌血症和死亡的明确危险因素,但它对接受长期血液透析(HD)患者的预后影响仍存在争议。
这项前瞻性干预性队列研究(2004 年至 2010 年进行)纳入了一家城市透析中心的 289 名 HD 门诊患者。所有患者初次入院、从其他透析机构转来或住院后再次入院时,均进行鼻拭子 MRSA 培养。对 MRSA 鼻腔携带者进行单间病房治疗,并给予莫匹罗星鼻软膏。同时,对其他部位的 MRSA 定植进行治疗,使用 0.2%洗必泰漱口液(喉咙)或含有奥替尼啶二盐酸盐的防腐肥皂和 2%洗必泰沐浴液(皮肤)。系统分析了携带者和非携带者的临床数据和结果。
筛查方法确定了 34 名鼻腔 MRSA 携带者(11.7%)。11/34(32%)的鼻腔 MRSA 携带者存在其他部位的 MRSA 定植。恶性肿瘤病史和增加的 Charlson 合并症指数是鼻腔 MRSA 携带者的显著预测因素,而传统的 MRSA 定植危险因素或炎症或营养不良标志物不能区分。Kaplan-Meier 分析表明,MRSA 携带者和非携带者之间的生存率存在显著差异。莫匹罗星软膏持续消除了 34 名患者中的 26 名(73.5%)鼻腔 MRSA 定植。未能成功清除鼻腔 MRSA 的持续携带者预后极差,全因死亡率>85%。
尽管缺乏明显的感染临床症状,但鼻腔 MRSA 定植并未能成功消除莫匹罗星,与死亡率增加相关。需要进一步的研究来证明鼻腔 MRSA 定植是否代表了 HD 患者预后更差的新预测因素,还是只是导致致命结局的合并症负担的另一个替代标志物。