Department of Rheumatology, Rheumazentrum Ruhrgebiet, , Herne, Germany.
Ann Rheum Dis. 2014 Jun;73(6):1107-13. doi: 10.1136/annrheumdis-2012-203075. Epub 2013 May 3.
To evaluate radiographic progression in patients with ankylosing spondylitis (AS) receiving two different doses of the tumour necrosis factor antagonist golimumab.
356 patients with AS were randomly assigned to placebo, or golimumab 50 mg or 100 mg every 4 weeks (wks). At wk16, patients with inadequate response early escaped with blinded dose adjustments (placebo→golimumab 50 mg, 50 mg→100 mg). At wk24, patients still receiving placebo crossed over to golimumab 50 mg. Lateral view radiographs of the cervical/lumbar spine were obtained at wk0, wk104 and wk208, and scored (two blinded readers, modified Stoke AS Spine Score (mSASSS)). Observed data were used for wk104 analyses; missing wk208 scores were linearly extrapolated.
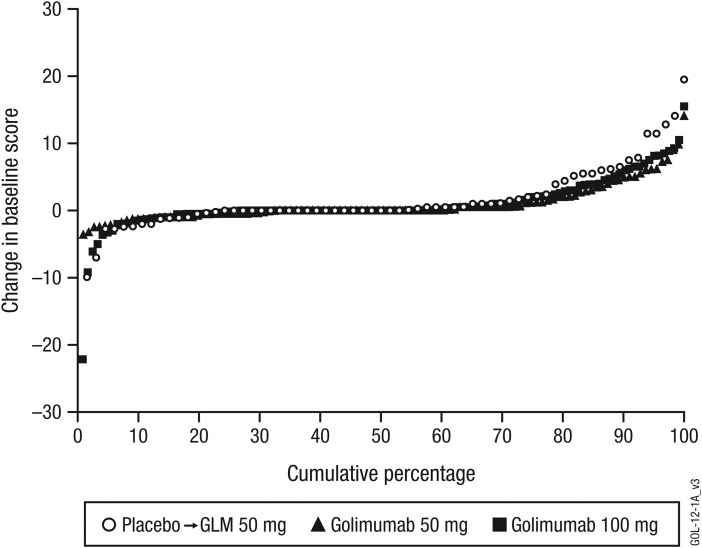
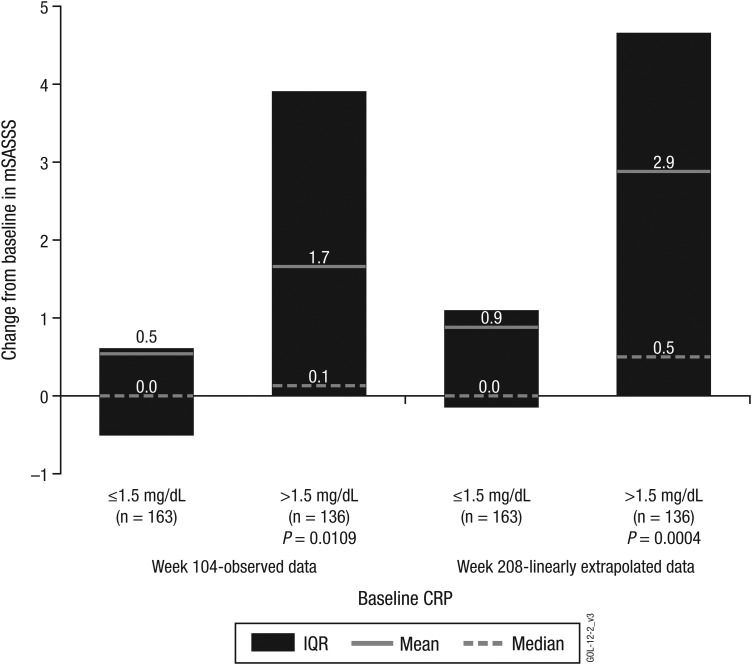
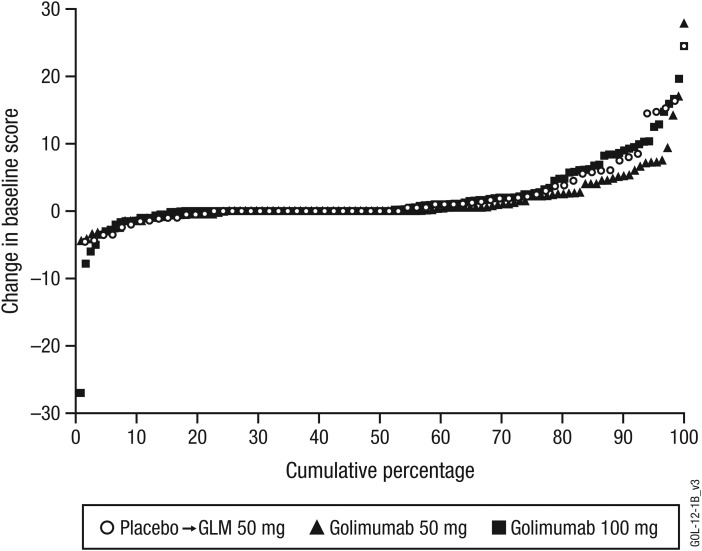
Wk104 changes from baseline in mSASSS averaged 1.6±4.6 for placebo crossover, 0.9±2.7 for 50 mg and 0.9±3.9 for 100 mg. By wk208, following golimumab therapy for 3.5-4 years, mean changes in mSASSS were 2.1±5.2 for placebo crossover, 1.3±4.1 for 50 mg and 2.0±5.6 for 100 mg. Less than a third of patients (placebo crossover, 19/66 (28.8%); 50 mg, 29/111 (26.1%); 100 mg, 35/122 (28.7%)) had a definitive change from baseline mSASSS (>2). Less radiographic progression was observed through wk208 in patients without baseline syndesmophytes (0.2 vs 2.8 in patients with ≥1 syndesmophyte; p<0.0001) and with baseline C-reactive protein (CRP) levels ≤1.5 mg/dl (0.9 vs 2.9 with CRP >1.5 mg/dl; p=0.0004).
No difference in mSASSS change was observed between golimumab 50 mg and 100 mg. The radiographic progression rate remained stable at years 2 and 4, suggesting no acceleration of new bone formation over time. Golimumab-treated AS patients with no syndesmophytes and less systemic inflammation at baseline had considerably less radiographic progression.
评估接受不同剂量肿瘤坏死因子拮抗剂戈利木单抗治疗的强直性脊柱炎(AS)患者的放射学进展。
356 例 AS 患者被随机分配至安慰剂组或戈利木单抗 50mg 或 100mg 每 4 周(wks)组。在第 16 周,早期应答不足的患者通过盲法剂量调整(安慰剂→戈利木单抗 50mg,50mg→100mg)提前逃逸。在第 24 周,仍接受安慰剂的患者交叉至戈利木单抗 50mg 组。在第 0、104 和 208 周时获取颈椎/腰椎的侧位 X 线片,并进行评分(两名盲法阅片者,改良 Stoke AS 脊柱评分(mSASSS))。采用观察数据进行第 104 周分析;缺失的第 208 周评分通过线性外推得出。
安慰剂交叉组第 104 周时 mSASSS 自基线的平均变化为 1.6±4.6,50mg 组为 0.9±2.7,100mg 组为 0.9±3.9。在接受戈利木单抗治疗 3.5-4 年后,第 208 周时 mSASSS 的平均变化为安慰剂交叉组 2.1±5.2,50mg 组 1.3±4.1,100mg 组 2.0±5.6。仅有不到三分之一的患者(安慰剂交叉组 19/66(28.8%);50mg 组 29/111(26.1%);100mg 组 35/122(28.7%))mSASSS 自基线有明确变化(>2)。与基线时存在骨桥(无骨桥患者 0.2 vs 有骨桥患者 2.8;p<0.0001)和基线 C 反应蛋白(CRP)水平≤1.5mg/dl(CRP>1.5mg/dl 患者 0.9 vs 2.9;p=0.0004)的患者相比,无骨桥患者和基线时全身炎症较轻的患者在第 208 周时放射学进展明显较少。
戈利木单抗 50mg 与 100mg 组的 mSASSS 变化无差异。在第 2 和第 4 年时,放射学进展率保持稳定,提示随时间推移没有新骨形成加速。基线时无骨桥且全身炎症较轻的戈利木单抗治疗的 AS 患者放射学进展显著较少。