Wild Aaron T, Ye Xiaobu, Ellsworth Susannah G, Smith Jessica A, Narang Amol K, Garg Tanu, Campian Jian, Laheru Daniel A, Zheng Lei, Wolfgang Christopher L, Tran Phuoc T, Grossman Stuart A, Herman Joseph M
The Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University School of Medicine, Baltimore, MD.
Am J Clin Oncol. 2015 Jun;38(3):259-65. doi: 10.1097/COC.0b013e3182940ff9.
Lymphopenia is a common consequence of chemoradiation therapy yet is seldom addressed clinically. This study was conducted to determine if patients with locally advanced pancreatic cancer (LAPC) treated with definitive chemoradiation develop significant lymphopenia and if this affects clinical outcomes.
A retrospective analysis of patients with LAPC treated with chemoradiation at a single institution from 1997 to 2011 was performed. Total lymphocyte counts (TLCs) were recorded at baseline and then monthly during and after chemoradiation. The correlation between treatment-induced lymphopenia, established prognostic factors, and overall survival was analyzed using univariate Cox regression analysis. Important factors identified by univariate analysis were selected as covariates to construct a multivariate proportional hazards model for survival.
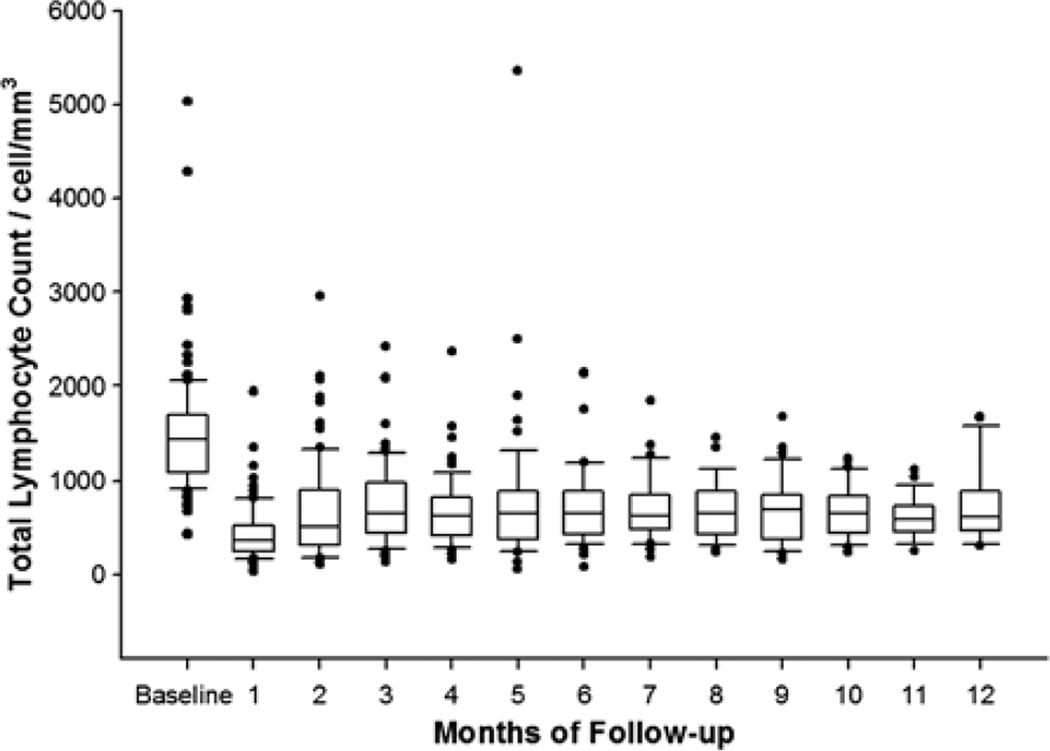
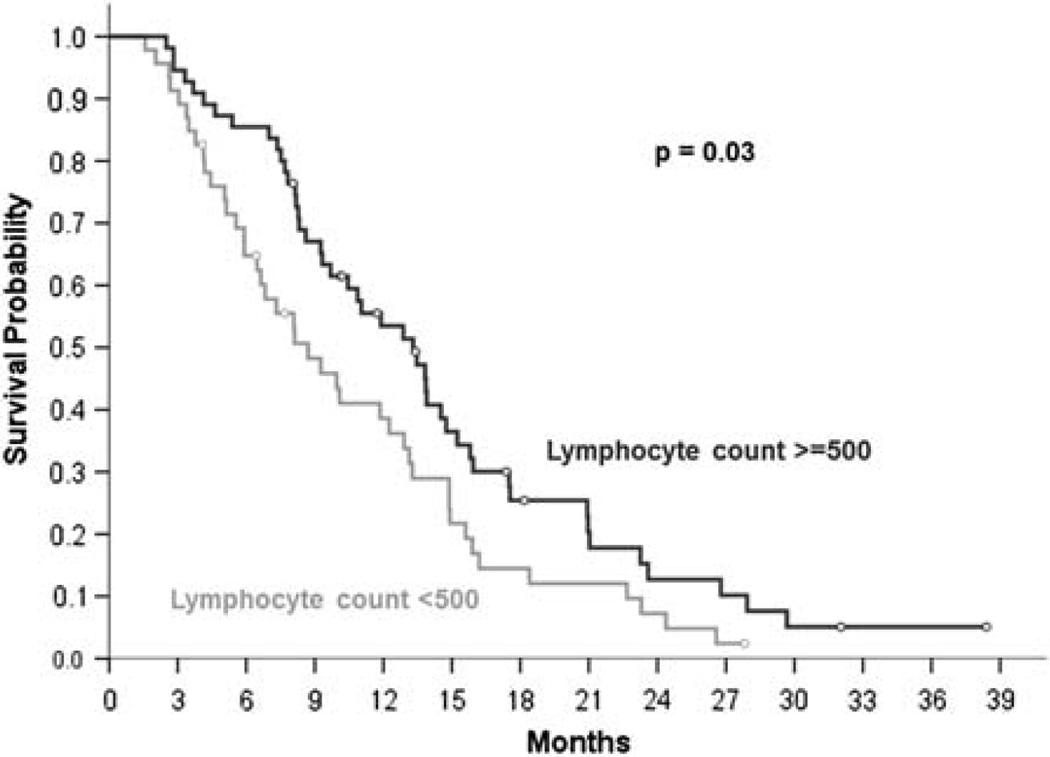
A total of 101 patients met eligibility criteria. TLCs were normal in 86% before chemoradiation. The mean reduction in TLC per patient was 50.6% (SD, 40.6%) 2 months after starting chemoradiation (P<0.00001), and 46% had TLC<500 cells/mm. Patients with TLC<500 cells/mm 2 months after starting chemoradiation had inferior median survival (8.7 vs. 13.3 mo, P=0.03) and PFS (4.9 vs. 9.0 mo, P=0.15). Multivariate analysis revealed TLC<500 cells/mm to be an independent predictor of inferior survival (HR=2.879, P=0.001) along with baseline serum albumin (HR=3.584, P=0.0002), BUN (HR=1.060, P=0.02), platelet count (HR=1.004, P=0.005), and radiation planning target volume (HR=1.003, P=0.0006).
Severe treatment-related lymphopenia occurs frequently after chemoradiation for LAPC and is an independent predictor of inferior survival.
淋巴细胞减少是放化疗常见的后果,但临床上很少对此加以关注。本研究旨在确定接受根治性放化疗的局部晚期胰腺癌(LAPC)患者是否会出现显著的淋巴细胞减少,以及这是否会影响临床结局。
对1997年至2011年在单一机构接受放化疗的LAPC患者进行回顾性分析。在基线时记录总淋巴细胞计数(TLC),然后在放化疗期间及之后每月记录一次。使用单变量Cox回归分析来分析治疗引起的淋巴细胞减少、既定预后因素与总生存期之间的相关性。单变量分析确定的重要因素被选作协变量,以构建生存的多变量比例风险模型。
共有101例患者符合入选标准。放化疗前86%的患者TLC正常。开始放化疗2个月后,每位患者TLC的平均降低幅度为50.6%(标准差,40.6%)(P<0.00001),46%的患者TLC<500个细胞/mm³。开始放化疗2个月后TLC<500个细胞/mm³的患者的中位生存期(8.7个月对13.3个月,P=0.03)和无进展生存期(4.9个月对9.0个月,P=0.15)较差。多变量分析显示,TLC<500个细胞/mm³是生存期较差的独立预测因素(风险比=2.879,P=0.001),同时还有基线血清白蛋白(风险比=3.584,P=0.0002)、血尿素氮(风险比=1.060,P=0.02)、血小板计数(风险比=1.004,P=0.005)和放射治疗计划靶体积(风险比=1.003,P=0.0006)。
LAPC放化疗后频繁发生严重的治疗相关淋巴细胞减少,且是生存期较差的独立预测因素。