Department of Radiation Oncology, Zhongshan Hospital, Fudan University, 180 Fenglin Road, Shanghai, 200032, China.
Radiat Oncol. 2019 May 27;14(1):86. doi: 10.1186/s13014-019-1287-z.
To investigate the potential impact of fractionation regimes and overall treatment time (OTT) on lymphopenia during definitive radiotherapy (RT) and its associations with patient outcomes in non-small cell lung cancer (NSCLC).
Subjects consisted of 115 patients who had received definitive chemoradiation therapy (CRT) with different doses and fractions for unresectable stage III NSCLC. Clinical and laboratory records were reviewed to assess the changes in total lymphocyte counts (TLCs) during definitive RT. The associations of the TLCs with the clinical and treatment features, and outcomes were analyzed.
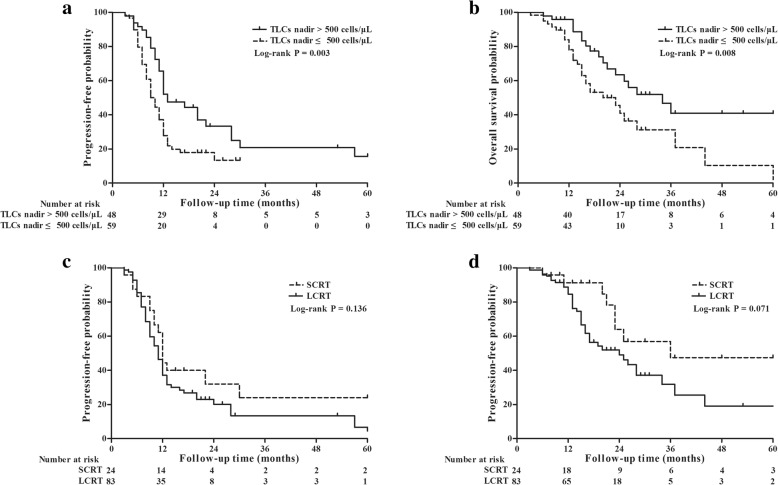
The median reduction of TLCs in the entire cohort was 1300 cells/μL (interquartile range [IQR], 950-1510 cells/μL). Of all patients, 63 (54.8%) experienced severe lymphopenia (SL) (TLC nadir < 500 cells/μL), which occurred at a median of the 5th week following RT initiation, not at the completion of RT or upon treatment with maximal doses. SL risk was increased over the first 5 weeks (odds ratio [OR] = 3.455, P = 0.007), after which, no increased risk was observed (OR = 0.562, P = 0.216). The median TLCs remained low and failed to recover to the initial normal values of their pre-RT level after 2 months of RT completion. Patients without SL exhibited significantly improved progression-free survival (hazard ratio [HR] = 0.544, P = 0.010) and overall survival (HR = 0.463, P = 0.011) after controlling for confounding variables in multivariate analyses. The incidence of SL was significantly lower (71.1% reduction in risk (OR = 0.289, P = 0.007)) in patients who received hypofractionated RT with an OTT within 4 weeks, compared to those who had an OTT of more than 4 weeks (32.1% vs 62.1%, P = 0.006). Multivariate analyses revealed that OTT within 4 weeks (OR = 0.322, P = 0.032) was significantly associated with a decreased risk of developing SL after controlling for confounding factors.
Hypofractionated RT was significantly associated with a decreased risk of SL and improved survival during definitive radiotherapy for unresectable stage III NSCLC.
本研究旨在探讨分割模式和总治疗时间(OTT)对不可切除 III 期非小细胞肺癌(NSCLC)根治性放疗期间淋巴细胞减少的潜在影响,并分析其与患者预后的相关性。
本研究纳入了 115 例接受根治性放化疗的不可切除 III 期 NSCLC 患者,这些患者接受了不同剂量和分割的治疗。回顾性分析临床和实验室记录,评估根治性放疗期间总淋巴细胞计数(TLC)的变化。分析 TLC 与临床和治疗特征及结局的相关性。
全队列中 TLC 的中位数下降了 1300 个细胞/μL(四分位距 [IQR],950-1510 个细胞/μL)。所有患者中,63 例(54.8%)发生严重淋巴细胞减少症(SL)(TLC 最低点<500 个细胞/μL),发生于放疗开始后第 5 周的中位数时间,而非放疗结束时或接受最大剂量时。在前 5 周内,SL 风险增加(优势比 [OR] = 3.455,P = 0.007),此后,风险未再增加(OR = 0.562,P = 0.216)。放疗完成后 2 个月,TLC 仍保持低值,未能恢复至放疗前的初始正常水平。多变量分析控制混杂变量后,无 SL 患者的无进展生存期(风险比 [HR] = 0.544,P = 0.010)和总生存期(HR = 0.463,P = 0.011)显著改善。与 OTT 超过 4 周的患者相比,接受 4 周内 OTT 的 HypoRT 患者的 SL 发生率显著降低(风险降低 71.1%(OR = 0.289,P = 0.007))(32.1% vs 62.1%,P = 0.006)。多变量分析显示,在控制混杂因素后,4 周内 OTT(OR = 0.322,P = 0.032)与 SL 发生风险降低显著相关。
对于不可切除 III 期 NSCLC 根治性放疗,HypoRT 与 SL 风险降低和生存改善显著相关。