Department of Radiation Oncology, MD Anderson Cancer Center Orlando, Orlando, FL 32806, USA.
J Appl Clin Med Phys. 2013 May 6;14(3):4210. doi: 10.1120/jacmp.v14i3.4210.
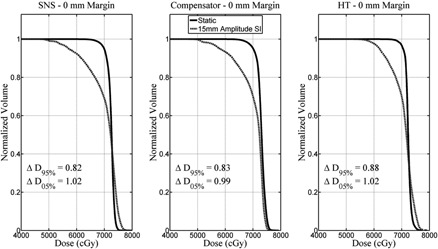
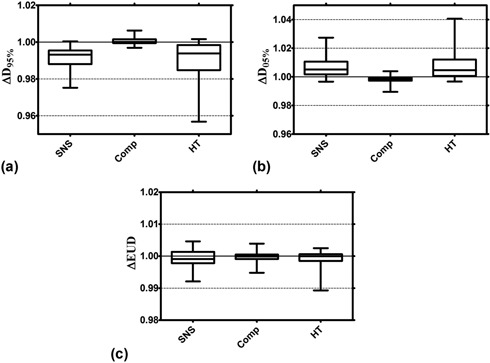
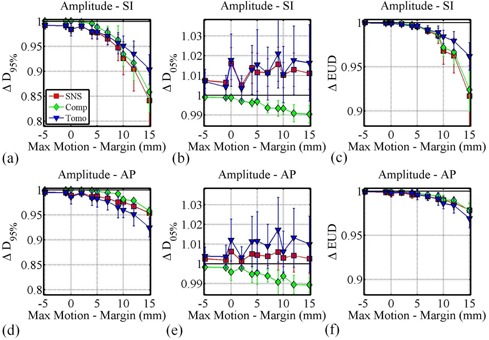
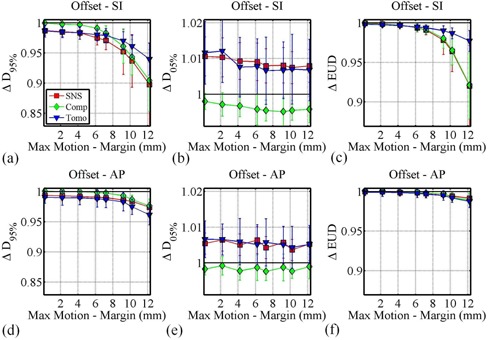
Intrafraction motion during intensity-modulated radiation therapy can cause differences between the planned and delivered patient dose. The magnitude of these differences is dependent on a number of variables, including the treatment modality. This study was designed to compare the relative susceptibility of plans generated with three different treatment modalities to intrafraction motion. The dosimetric effects of motion were calculated using computational algorithms for seven lung tumor patients. Three delivery techniques - MLC-based step-and-shoot (SNS), beam attenuating compensators, and helical tomotherapy (HT) - were investigated. In total 840 motion-encoded dose-volume histograms (DVHs) were calculated for various combinations of CTV margins and sinusoidal CTV motion including CTV offsets. DVH-based metrics (e.g., D95% and D05%) were used to score plan degradations. For all three modalities, dosimetric degradations were typically smaller than 3% if the CTV displacement was smaller than the CTV margin. For larger displacements, technique and direction-specific sensitivities existed. While the HT plans show similar D95% degradations for motion in the SI and AP directions, SNS and compensator plans showed larger D95% degradations for motion in the SI direction than for motion in the AP direction. When averaged over all motion/margin combinations, compensator plans resulted in 0.9% and 0.6% smaller D95% reductions compared to SNS and HT plans, respectively. These differences were statistically significant. No statistically significant differences in D95% degradations were found between SNS and HT for data averaged over all margin and motion track combinations. For CTV motion that is larger than the CTV margin, the dosimetric impact on the CTV varies with treatment technique and the motion direction. For the cases presented here, the effect of motion on CTV dosimetry was statistically smaller for compensator deliveries than SNS and HT, likely due to the absence of the interplay effect which is present for the more dynamic treatment deliveries. The differences between modalities were, however, small and might not be clinically significant. As expected, margins that envelop the CTV motion provide dosimetric protection against motion for all three modalities.
调强放疗过程中的分次内运动可能导致计划剂量与实际剂量之间存在差异。这些差异的大小取决于许多变量,包括治疗方式。本研究旨在比较三种不同治疗方式生成的计划对分次内运动的相对敏感性。使用计算算法为 7 名肺癌患者计算了运动的剂量学效应。研究了三种输送技术:基于多叶准直器的步进式(SNS)、射束衰减补偿器和螺旋断层放疗(HT)。总共为不同的CTV 边界和包括 CTV 偏移的正弦CTV 运动组合计算了 840 个运动编码剂量-体积直方图(DVH)。基于 DVH 的指标(例如,D95%和 D05%)用于评估计划降级。对于所有三种方式,如果 CTV 位移小于 CTV 边界,则剂量学降级通常小于 3%。对于较大的位移,存在与技术和方向相关的敏感性。虽然 HT 计划在 SI 和 AP 方向的运动中显示出相似的 D95%降级,但 SNS 和补偿器计划在 SI 方向的运动中比在 AP 方向的运动中显示出更大的 D95%降级。当平均所有运动/边界组合时,补偿器计划导致 D95%减少分别比 SNS 和 HT 计划小 0.9%和 0.6%。这些差异具有统计学意义。对于平均所有边界和运动轨迹组合的数据,SNS 和 HT 之间的 D95%降级没有统计学上的显著差异。对于大于 CTV 边界的 CTV 运动,治疗技术和运动方向会对 CTV 的剂量学产生影响。对于这里呈现的情况,由于不存在适用于更动态治疗输送的相互作用效应,补偿器输送对 CTV 剂量学的影响在统计学上小于 SNS 和 HT,这可能是由于不存在适用于更动态治疗输送的相互作用效应。然而,不同方式之间的差异很小,可能没有临床意义。正如预期的那样,包围 CTV 运动的边界为所有三种方式提供了针对运动的剂量学保护。