Department of Surgery, Washington University School of Medicine, St. Louis, Missouri, USA.
Ann Thorac Surg. 2013 Aug;96(2):382-90. doi: 10.1016/j.athoracsur.2013.03.093. Epub 2013 May 31.
Clinical staging of esophageal cancer has improved with positron-emission tomography/computed tomography and endoscopic ultrasound imaging. Despite such progress, small single-center studies have questioned the reliability of clinical staging of T2 N0 esophageal cancer. This study broadly examines the adequacy of clinical staging of T2 N0 disease using The Society of Thoracic Surgeons database.
We retrospectively studied 810 clinical stage T2 N0 patients from 2002 to 2011, with 58 excluded because of incomplete pathologic staging data. Clinical stage, pathologic stage, and preoperative characteristics were recorded. Logistic regression analysis was used to identify factors associated with upstaging at the time of surgical intervention.
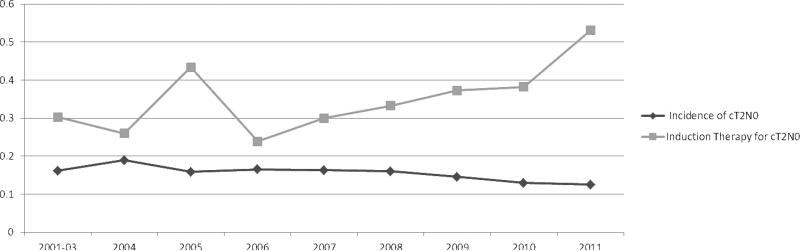
Among 752 clinical stage T2 N0 patients, 270 (35.9%) received induction therapy before the operation. Of 482 patients who went directly to surgical intervention, 132 (27.4%) were confirmed as pathologic T2 N0, 125 (25.9%) were downstaged (ie, T0-1 N0), and 225 (46.7%) were upstaged at the operation (T3-4 N0 or Tany N1-3). Exclusive tumor upstaging (ie, pathologic T3-4 N0) accounted for 41 patients (18.2%), whereas exclusive nodal upstaging (ie, pathological T1-2 N1-3) accounted for 100 (44.5%). Combined tumor and nodal upstaging (ie, pathological T3-4 N1-3) accounted for 84 patients (37.3%). Among patients who received induction therapy, 103 (38.1%) were upstaged vs 225 (46.7%) without induction therapy (p = 0.026). Comparing the induction therapy group and the primary surgical group, postoperative 30-day mortality (3.7% vs 3.7%, p > 0.99) and morbidity (46.3% vs 45%, p = 0.76) were similar.
Despite advances in staging techniques, clinical staging of T2 N0 esophageal cancer remains unreliable. Recognizing T2 N0 as a threshold for induction therapy in esophageal cancer, many surgeons have opted to treat T2 N0 disease with induction therapy, even though one-quarter of these patients will be pathologic T1 N0. Although this study demonstrated similar perioperative morbidity and mortality with and without induction therapy, further study is needed to examine the effect of upstaging on long-term survival.
正电子发射断层扫描/计算机断层扫描和内镜超声成像提高了食管癌的临床分期。尽管取得了这些进展,但一些小型单中心研究对 T2N0 食管癌临床分期的可靠性提出了质疑。本研究广泛地使用胸外科医师协会数据库来检查 T2N0 疾病的临床分期是否充分。
我们回顾性研究了 2002 年至 2011 年间的 810 例临床分期为 T2N0 的患者,其中 58 例因病理分期资料不完整而被排除在外。记录了临床分期、病理分期和术前特征。采用 logistic 回归分析确定与手术干预时分期升级相关的因素。
在 752 例临床分期为 T2N0 的患者中,有 270 例(35.9%)在手术前接受了诱导治疗。在 482 例直接接受手术干预的患者中,有 132 例(27.4%)被确认为病理 T2N0,125 例(25.9%)降期(即 T0-1N0),225 例(46.7%)升级(即 T3-4N0 或任何 N1-3)。肿瘤单纯升级(即病理 T3-4N0)占 41 例(18.2%),而淋巴结单纯升级(即病理 T1-2N1-3)占 100 例(44.5%)。肿瘤和淋巴结同时升级(即病理 T3-4N1-3)占 84 例(37.3%)。在接受诱导治疗的患者中,有 103 例(38.1%)升级,而未接受诱导治疗的患者有 225 例(46.7%)(p=0.026)。与接受诱导治疗的患者相比,接受诱导治疗组和直接手术组的术后 30 天死亡率(3.7%比 3.7%,p>0.99)和发病率(46.3%比 45%,p=0.76)相似。
尽管分期技术有所进步,但 T2N0 食管癌的临床分期仍然不可靠。将 T2N0 视为食管癌诱导治疗的阈值,许多外科医生选择对 T2N0 疾病进行诱导治疗,尽管其中四分之一的患者病理分期为 T1N0。尽管本研究表明诱导治疗组和非诱导治疗组的围手术期发病率和死亡率相似,但仍需要进一步研究分期升级对长期生存的影响。