Organ Transplant Department, Saint Petersburg Pavlov State Medical University, Saint Petersburg, Russia.
PLoS One. 2013 May 30;8(5):e64209. doi: 10.1371/journal.pone.0064209. Print 2013.
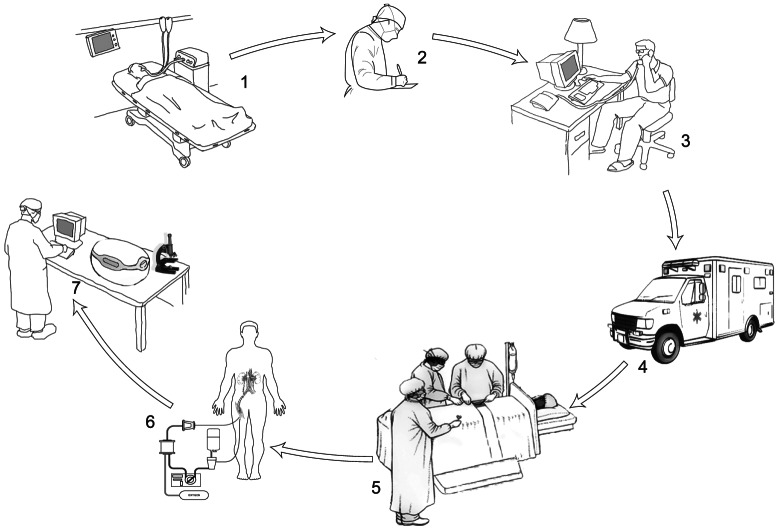
Organ shortage leads to usage of kidneys from donors after sudden cardiac death, or uncontrolled donors (UDCD). Ischemic injury due to cessation of circulation remains a crucial problem that limits adoption of UDCD. Our clinical investigation was to determine the applicability of kidneys obtained from UDCD and resuscitated by extracorporeal perfusion in situ after 60 minutes of asystole.
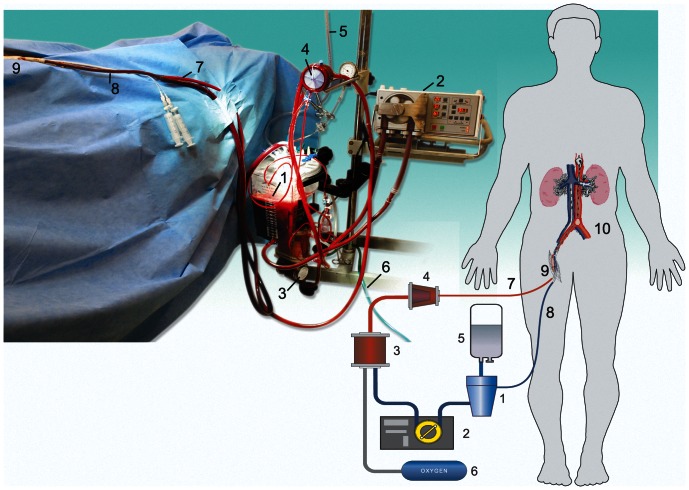
In 2009-2011, organ procurement service of St. Petersburg, obtained kidneys from 22 UDCD with critically expanded warm ischemic time (WIT). No patients were considered as potential organ donors initially. All donors died after sudden irreversible cardiac arrest. Mean WIT was 61.4±4.5 minutes. For kidney resuscitation, the subnormothermic extracorporeal abdominal perfusion with thrombolytics and leukocyte depletion was employed. Grafts were transplanted into 44 recipients. The outcomes of transplantation of resuscitated kidneys were compared to outcomes of 87 KTx from 74 brain death donors (BDDs).
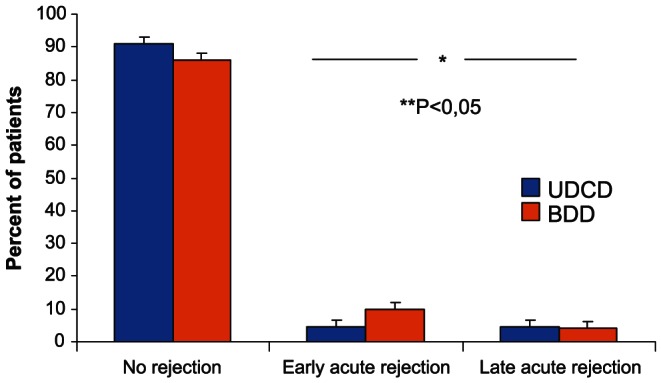
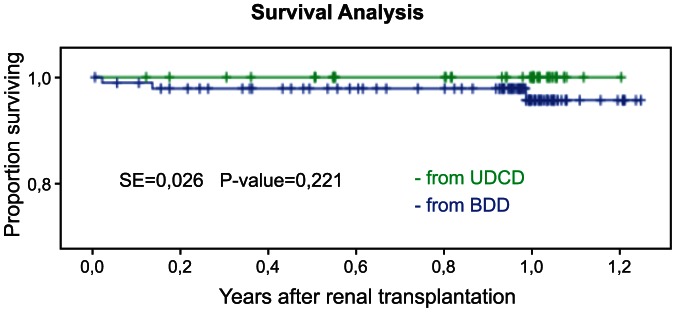
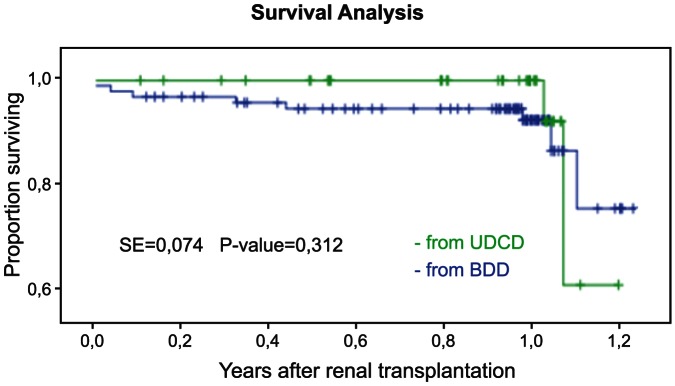
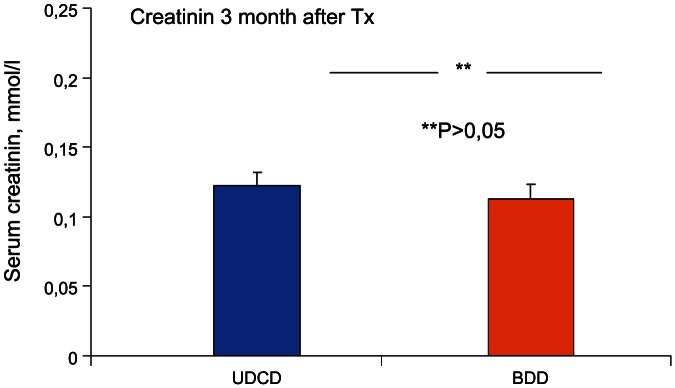
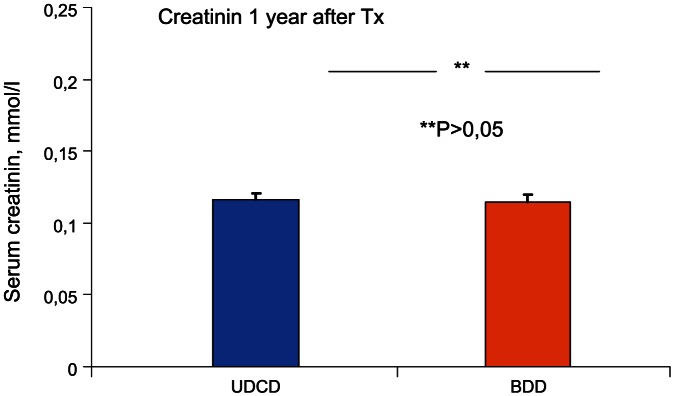
Immediate functioning of kidney grafts was observed in 21 of the 44 recipients, with no cases of primary non function. By the end of the first post-transplant year there was an acute rejection rate of 9.1% (4 episodes of rejection) in the UDCD group versus 14.2% (13 episodes of rejection) in the BDD group. The actual 1-year graft survival rate was 95.5% (n = 42) in UDCD group, and 94.6% (n = 87) in BDD group. Creatinine levels at the end of the first year were 0.116±0.008 and 0.115±0.004 mmol/l in UDCD and BDD groups, respectively.
UDCD kidneys with critically expanded WIT could be succefully used for transplantation if in situ organ "resuscitation" perfusion is included into procurement protocol. The results of 1-year follow-up meet the generally accepted criteria for graft survival and function. In situ reperfusion may exert a therapeutic effect on grafts before procurement. This approach could substantially expand the organ donors' pool.
由于器官短缺,人们开始使用心脏停搏后或非控制性供体(UDCD)的肾脏。由于血液循环停止导致的缺血性损伤仍然是限制采用 UDCD 的一个关键问题。我们的临床研究旨在确定在心脏停搏 60 分钟后通过体外灌注原位复苏获得的 UDCD 肾脏的适用性。
2009 年至 2011 年,圣彼得堡的器官获取服务机构从 22 例具有严重扩展热缺血时间(WIT)的 UDCD 中获得了肾脏。最初并没有考虑这些患者作为潜在的器官捐献者。所有供体均在突发不可逆性心脏骤停后死亡。平均 WIT 为 61.4±4.5 分钟。为了使肾脏复苏,采用低温体外腹部灌注溶栓和白细胞耗竭的方法。将移植物移植到 44 例受者中。将复苏肾脏的移植结果与 74 例脑死亡供体(BDD)的 87 例 KTx 的移植结果进行了比较。
44 例受者中有 21 例即刻肾功能正常,没有发生原发性无功能。在移植后的第一年结束时,UDCD 组有 9.1%(4 例排斥反应)发生急性排斥反应,而 BDD 组有 14.2%(13 例排斥反应)。UDCD 组的实际 1 年移植物存活率为 95.5%(n=42),BDD 组为 94.6%(n=87)。在第一年结束时,UDCD 组和 BDD 组的肌酐水平分别为 0.116±0.008 和 0.115±0.004mmol/L。
如果将器官“复苏”灌注纳入采购方案,可成功使用 WIT 严重扩展的 UDCD 肾脏进行移植。1 年随访结果符合公认的移植物存活率和功能标准。原位再灌注可能在采购前对移植物产生治疗作用。这种方法可以大大扩大器官捐献者的范围。