Health Economics, United BioSource Corporation, 7101 Wisconsin Avenue, Suite 600, Bethesda, MD 20814, USA.
Adv Ther. 2013 May;30(5):517-27. doi: 10.1007/s12325-013-0034-3. Epub 2013 Jun 6.
Dose escalation with tumor necrosis factor (TNF)-blockers is poorly characterized in pharmacy benefit management (PBM) settings.
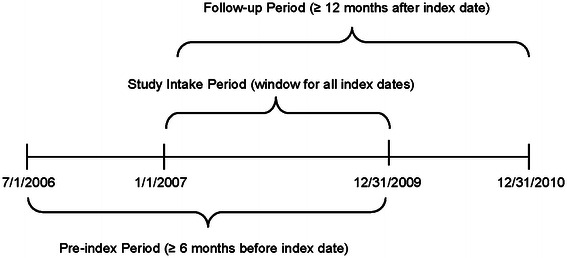
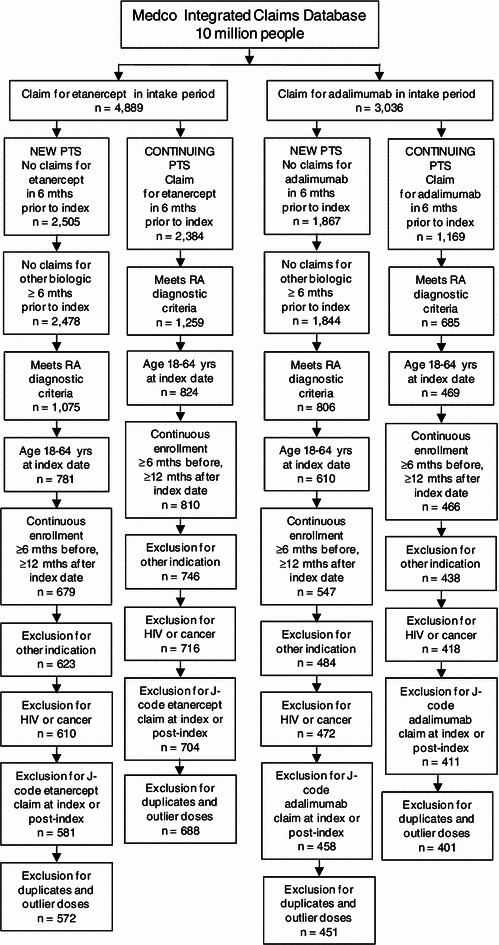
This retrospective study used integrated pharmacy and medical claims from the PBM Medco to characterize dose escalation among rheumatoid arthritis (RA) patients treated with etanercept and adalimumab. Data from adults with RA with pharmacy claims for etanercept or adalimumab between 1/1/2007 and 12/31/2009 and continuous enrollment for ≥ 6 months before and ≥ 12 months after first (index) pharmacy claim were analyzed. "New" patients had no claim for TNF-blocker in the 6 months prior to receipt of their index TNF-blocker; otherwise, they were classified as "continuing" patients. Endpoints included 12-month persistence and duration on index medication and dose escalation. Dose escalation (allowed per adalimumab label but not for etanercept) in patients' persistent ≥ 12 months was estimated using five methods: (1) average weekly dose ≥ 110% of recommended label dose; (2) average subsequent dose ≥ 130% of starting dose; (3) last dose ≥ 110% of starting dose; (4) ≥ 2 consecutive instances of dose ≥ 130% of starting dose; and (5) any instance where dose increase connoted an additional syringe/vial use.
Data from 1,260 patients on etanercept and 852 patients on adalimumab were analyzed; 45.3 and 45.9% of new patients on etanercept and adalimumab, respectively, and 60.5 and 60.8% of continuing patients had ≥ 12 months persistence on index medication. Across all five methods used to estimate dose escalation, patients receiving etanercept had significantly lower rates of dose escalation (P < 0.001) than patients receiving adalimumab. For new patients, rates of dose escalation were 0.4-1.2% for etanercept and 8.3-14.1% for adalimumab. For continuing patients, rates ranged from 1.1 to 2.9% for etanercept and 7.0-28.3% for adalimumab.
New and continuing patients from this PBM database on etanercept had significantly lower rates of dose escalation than patients on adalimumab.
在药品福利管理(PBM)环境中,肿瘤坏死因子(TNF)阻滞剂的剂量升级情况描述得并不充分。
本回顾性研究使用 PBM Medco 的综合药房和医疗索赔数据,描述了接受依那西普和阿达木单抗治疗的类风湿关节炎(RA)患者的剂量升级情况。数据分析纳入了在 2007 年 1 月 1 日至 2009 年 12 月 31 日期间有依那西普或阿达木单抗药房索赔记录,且在首次(索引)药房索赔前至少 6 个月和之后至少 12 个月持续有医疗保险的成年 RA 患者。“新”患者在接受索引 TNF 阻滞剂前的 6 个月内没有 TNF 阻滞剂的索赔;否则,他们被归类为“持续”患者。终点包括 12 个月的持续用药和索引药物的用药时间,以及剂量升级。对持续用药时间≥12 个月的患者,采用五种方法估计剂量升级:(1)平均每周剂量≥推荐标签剂量的 110%;(2)平均后续剂量≥起始剂量的 130%;(3)末次剂量≥起始剂量的 110%;(4)≥2 次剂量≥起始剂量的 130%;(5)剂量增加表示额外使用 1 支/瓶的任何情况。
共分析了 1260 例依那西普和 852 例阿达木单抗患者的数据;新患者中,分别有 45.3%和 45.9%的依那西普和阿达木单抗患者、持续患者中,分别有 60.5%和 60.8%的依那西普和阿达木单抗患者在索引药物上有≥12 个月的持续用药时间。在所有五种用于估计剂量升级的方法中,接受依那西普治疗的患者剂量升级率显著低于接受阿达木单抗治疗的患者(P<0.001)。对于新患者,依那西普的剂量升级率为 0.4%-1.2%,阿达木单抗的剂量升级率为 8.3%-14.1%。对于持续患者,依那西普的剂量升级率为 1.1%-2.9%,阿达木单抗的剂量升级率为 7.0%-28.3%。
从这个 PBM 数据库来看,接受依那西普治疗的新患者和持续患者的剂量升级率明显低于接受阿达木单抗治疗的患者。