Department of Anesthesiology, Vanderbilt University School of Medicine, Nashville, TN, USA Department of Behavioral Science, Rush University, Chicago, IL, USA Department of Anesthesiology, Rush University, Chicago, IL, USA Department of Psychology, Ohio University, Athens, OH, USA.
Pain. 2013 Sep;154(9):1856-1864. doi: 10.1016/j.pain.2013.06.002. Epub 2013 Jun 6.
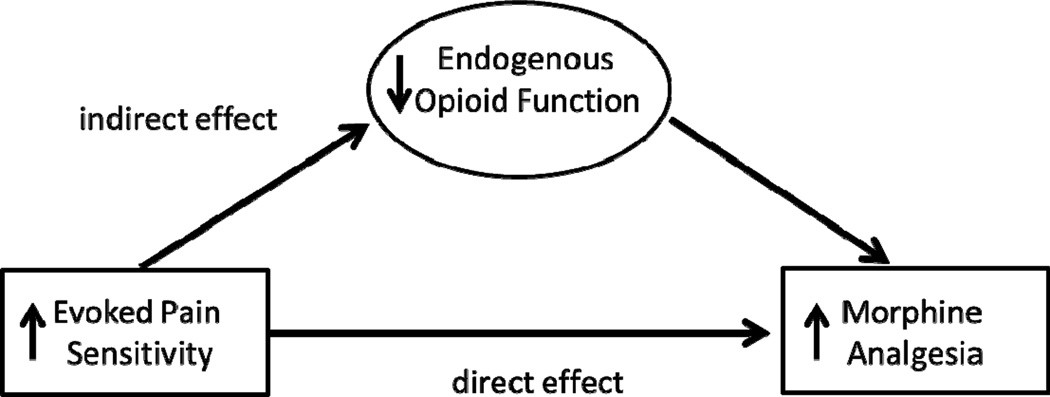
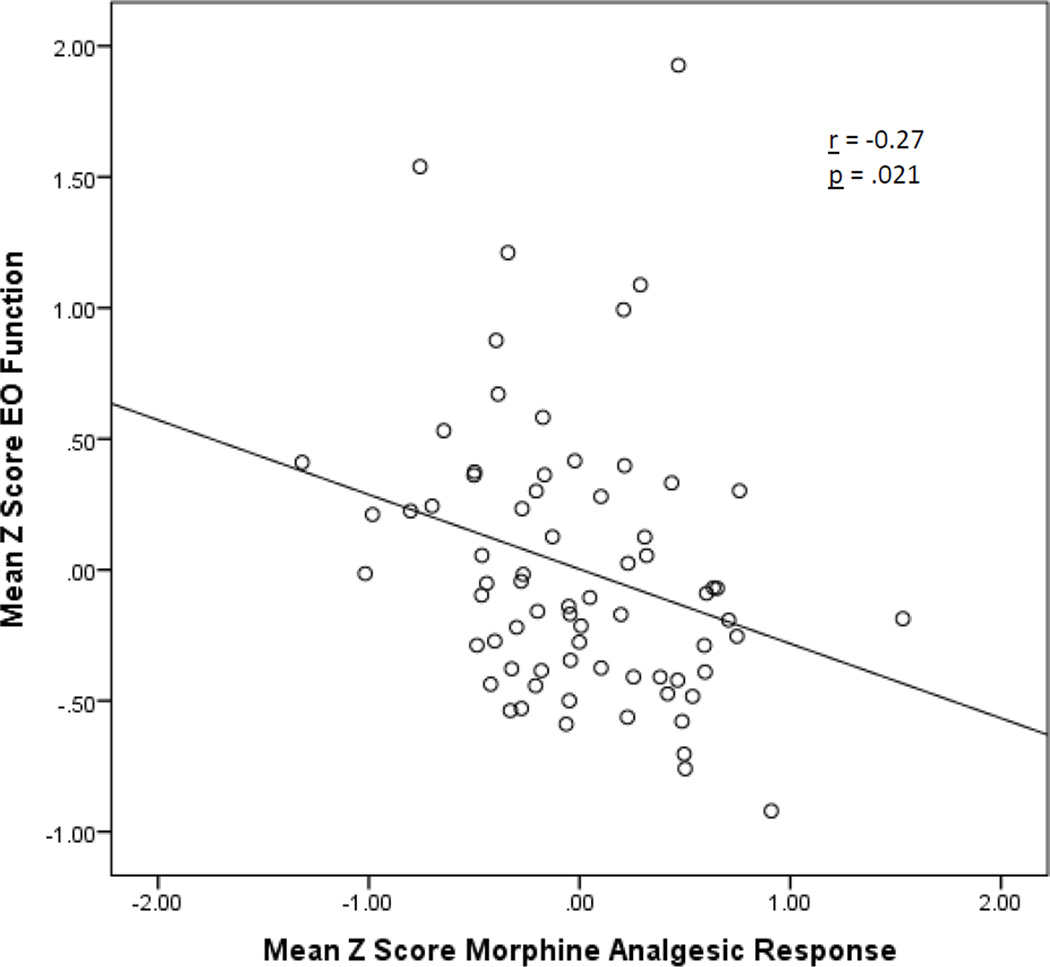
Predictors of responsiveness to opioid analgesic medications are not well understood. This study tested whether individual differences in endogenous opioid (EO) function are associated with analgesic responsiveness to morphine. In randomized, counterbalanced order over 3 sessions, 45 chronic low back pain participants and 31 healthy controls received an opioid antagonist (8 mg naloxone), morphine (0.08 mg/kg), or placebo. Participants then engaged in 2 laboratory-evoked pain tasks (ischemic and thermal). Outcomes included pain threshold, pain tolerance, and pain ratings. Indexes of EO function and morphine analgesic responsiveness were derived for each measure as the difference in pain responses between the placebo condition and naloxone or morphine condition, respectively. For all 7 pain measures across the 2 laboratory pain tasks, greater EO function was associated with significantly lower morphine analgesic responsiveness (P<0.001-P=0.02). Morphine reduced pain responses of low EO individuals to levels similar to those of high EO individuals receiving placebo. Higher placebo condition-evoked pain sensitivity was associated with significantly greater morphine analgesic responsiveness for 5 of 7 pain measures (P<0.001-P=0.02). These latter associations were significantly mediated by EO function for 4 of these 5 pain outcomes (all P values<0.05). In the laboratory-evoked pain context, opioid analgesic medications may supplement inadequate EO analgesia, with little incremental benefit in those with preexisting high EO function. Implications for personalized medicine are discussed.
阿片类镇痛药物的反应性预测因素尚不清楚。本研究旨在检验内源性阿片(EO)功能的个体差异是否与吗啡的镇痛反应性相关。45 名慢性腰痛患者和 31 名健康对照者被随机分为 3 组,在 3 个不同的时间段内分别接受了阿片受体拮抗剂(8mg 纳洛酮)、吗啡(0.08mg/kg)或安慰剂。然后,参与者参与了 2 项实验室诱发的疼痛任务(缺血性和热刺激)。结果包括疼痛阈值、疼痛耐受度和疼痛评分。EO 功能和吗啡镇痛反应性的指标分别是安慰剂条件和纳洛酮或吗啡条件下疼痛反应的差异。在 2 项实验室疼痛任务的 7 项疼痛测量中,EO 功能越高,吗啡镇痛反应性越低(P<0.001-P=0.02)。吗啡降低了低 EO 个体的疼痛反应,使其疼痛水平与接受安慰剂的高 EO 个体相似。较高的安慰剂条件下诱发的疼痛敏感性与 7 项疼痛测量中的 5 项有显著的更大的吗啡镇痛反应性相关(P<0.001-P=0.02)。对于这 5 项疼痛结果中的 4 项,这些关联均显著被 EO 功能所介导(所有 P 值<0.05)。在实验室诱发的疼痛环境中,阿片类镇痛药物可能会补充不足的 EO 镇痛作用,而对于原本 EO 功能较高的个体,其益处不大。文中讨论了个性化医疗的意义。