Department of Pharmaceutical Sciences, St. Jude Children's Research Hospital, 262 Danny Thomas Place, Memphis, TN 38105-3678, USA.
Cancer Chemother Pharmacol. 2013 Aug;72(2):369-78. doi: 10.1007/s00280-013-2206-x. Epub 2013 Jun 13.
It is advantageous to individualize high-dose methotrexate (HDMTX) to maintain adequate exposure while minimizing toxicities. Previously, we accomplished this through within-course dose adjustments.
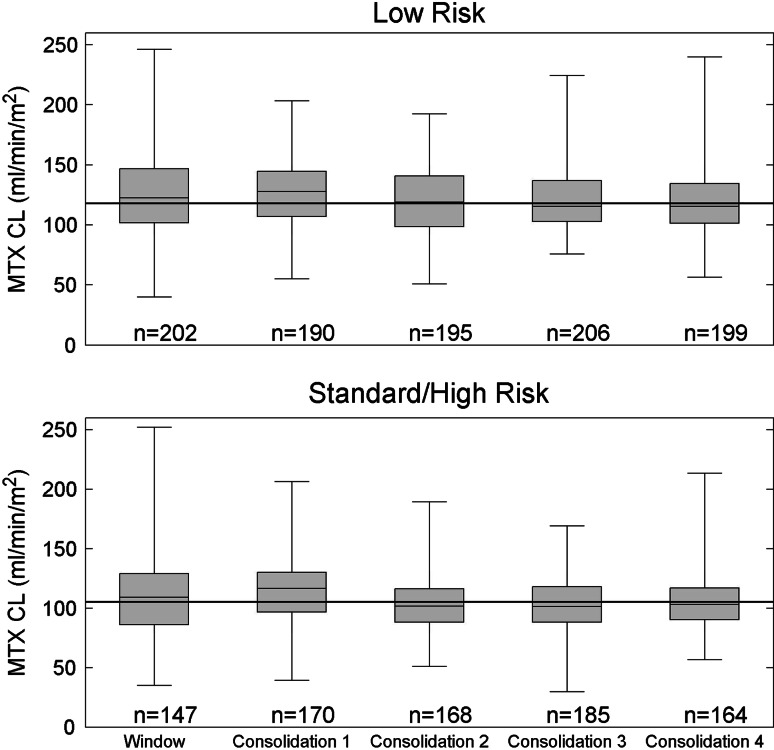
In this study, we evaluated a strategy to individualize HDMTX based on clearance of each individual's previous course of HDMTX in 485 patients with newly diagnosed acute lymphoblastic leukemia. Doses were individualized to achieve a steady-state plasma concentration (Cpss) of 33 or 65 μM (approximately 2.5 or 5 g/m(2)/day) for low- and standard-/high-risk patients, respectively.
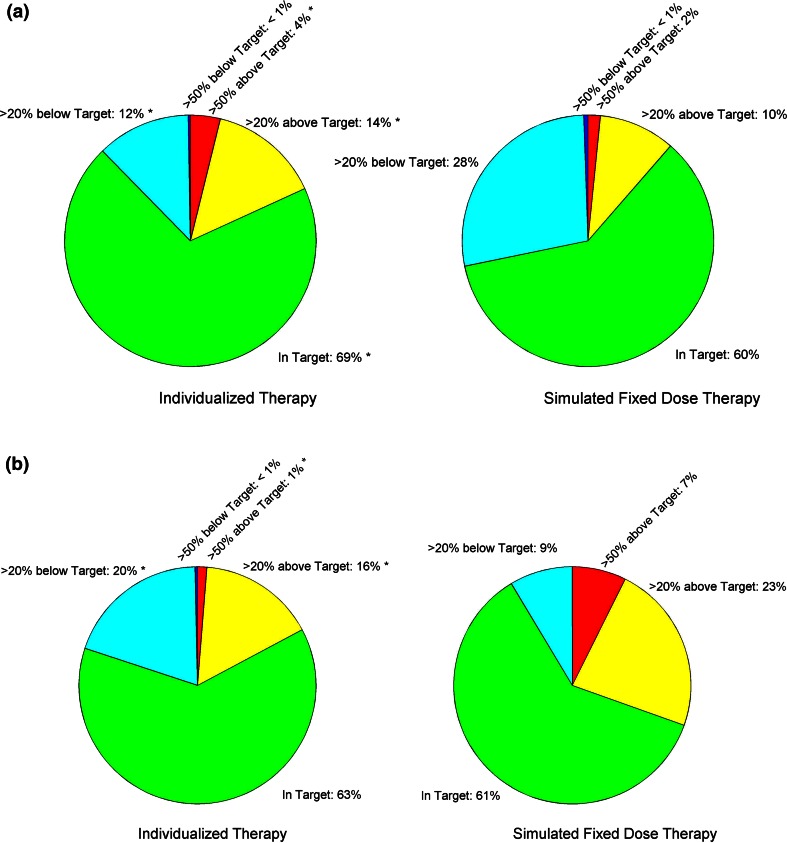
Individualized doses resulted in 70 and 63 % of courses being within 20 % of the targeted Cpss in the low- and standard-/high-risk arms, respectively, compared to 60 % (p < 0.001) and 61 % (p = 0.43) with conventionally dosed therapy. Only 1.3 % of the individualized courses in the standard-/high-risk arm had a Cpss greater than 50 % above the target compared to 7.3 % (p < 0.001) in conventionally dosed therapy. We observed a low rate (8.5 % of courses) of grade 3-4 toxicities. The odds of gastrointestinal toxicity were related to methotrexate plasma concentrations in both the low (p = 0.021)- and standard-/high-risk groups (p = 0.003).
Individualizing HDMTX based on the clearance from the prior course resulted in fewer extreme Cpss values and less delayed excretion compared to conventional dosing.
通过剂量调整实现个体化大剂量甲氨蝶呤(HDMTX)治疗,在降低毒性的同时保证充分暴露。
本研究通过对 485 例初诊急性淋巴细胞白血病患者前一疗程 HDMTX 清除率进行评估,建立了一种基于个体的个体化 HDMTX 策略。为低危、中危/高危患者设定个体化剂量,以实现稳态血药浓度(Css)分别为 33 或 65 μM(分别约为 2.5 或 5 g/m2/天)。
与传统剂量相比,个体化剂量使低危和中危/高危组分别有 70%和 63%的疗程 Css 处于目标值的 20%以内,而传统剂量分别为 60%(p<0.001)和 61%(p=0.43)。在中危/高危组,仅有 1.3%的个体化疗程 Css 超过目标值 50%,而传统剂量为 7.3%(p<0.001)。我们观察到,中危/高危组的 3-4 级毒性发生率较低(8.5%的疗程)。胃肠道毒性的发生风险与低危(p=0.021)和中危/高危组(p=0.003)的甲氨蝶呤血药浓度相关。
与传统剂量相比,基于前一疗程清除率进行个体化 HDMTX 治疗可降低血药浓度极端值和延迟排泄的发生率。