Duke Clinical Research Institute, Durham, North Carolina 27715, USA.
Heart Rhythm. 2013 Aug;10(8):1127-33. doi: 10.1016/j.hrthm.2013.06.009. Epub 2013 Jun 14.
A 2008 expert consensus statement recommended an in-person follow-up visit between 2 and 12 weeks after the placement of a new cardiovascular implantable electronic device (CIED).
To assess outcomes associated with adherence to the experts' recommendations.
By using data from the National Cardiovascular Data Registry's (NCDR) ICD Registry linked to Medicare claims, we studied the association between follow-up within 2-12 weeks after CIED placement between January 1, 2005, and September 30, 2008, and all-cause mortality and risk of readmission within 1 year.
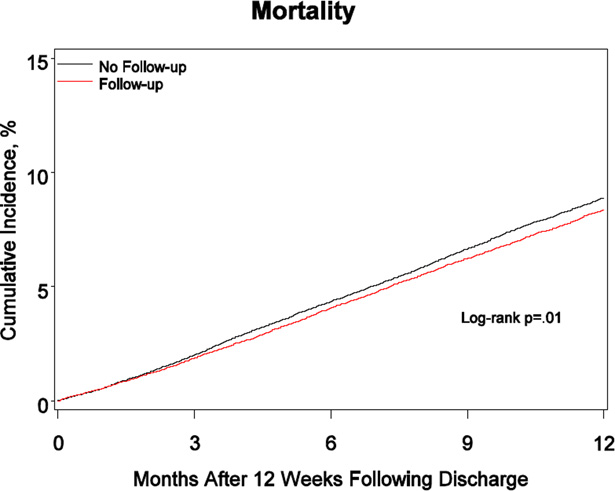
Compared with patients who did not receive the recommended follow-up (n = 43,060), those who did (n = 30,256) were more likely to be older, white, to have received a cardiac resynchronization therapy-defibrillator device, to have more advanced heart failure symptoms, and to have nonischemic dilated cardiomyopathy. In Cox proportional hazards models adjusted for patient demographic and clinical factors, mortality was lower (hazard ratio [HR] 0.93; 95% confidence interval [CI] 0.88-0.98; P = .005) but cardiovascular readmission was higher (HR 1.04; 95% CI 1.01-1.08; P = .012) among patients who received initial follow-up within 2-12 weeks after CIED placement compared with those who did not. There was no association between CIED follow-up and readmission for heart failure (HR 1.00; 95% CI 0.96-1.05; P = .878) or device-related infection (HR 1.22; 95% CI 0.98-1.51; P = .075).
Follow-up within 2-12 weeks after CIED placement was independently associated with improved survival but increased cardiovascular readmission. Quality improvement initiatives designed to increase adherence to experts' recommendations may be warranted.
2008 年的一份专家共识建议,在植入新的心血管植入式电子设备(CIED)后 2 至 12 周内进行面对面随访。
评估遵循专家建议的结果。
利用国家心血管数据注册中心(NCDR)的 ICD 注册数据与医疗保险索赔数据的关联,我们研究了 2005 年 1 月 1 日至 2008 年 9 月 30 日期间,CIED 植入后 2-12 周内进行随访与 1 年内全因死亡率和再入院风险之间的关系。
与未接受推荐随访的患者(n = 43060)相比,接受推荐随访的患者(n = 30256)年龄更大、更可能为白人、接受心脏再同步治疗除颤器装置、心力衰竭症状更严重、患有非缺血性扩张型心肌病。在调整患者人口统计学和临床因素的 Cox 比例风险模型中,接受初始随访的患者死亡率较低(风险比 [HR] 0.93;95%置信区间 [CI] 0.88-0.98;P =.005),但心血管再入院率较高(HR 1.04;95% CI 1.01-1.08;P =.012)。CIED 随访与心力衰竭再入院(HR 1.00;95% CI 0.96-1.05;P =.878)或器械相关感染(HR 1.22;95% CI 0.98-1.51;P =.075)之间无关联。
CIED 植入后 2-12 周内进行随访与生存改善独立相关,但心血管再入院率增加。可能需要设计提高对专家建议的依从性的质量改进计划。