Federal University of Ouro Preto, Department of Medical Sciences, Ouro Preto/MG, Brazil.
Clinics (Sao Paulo). 2013 May;68(5):612-20. doi: 10.6061/clinics/2013(05)06.
We conducted a study to identify gender differences in factors associated with the first episode of non-adherence in the 12 months following the first antiretroviral prescription.
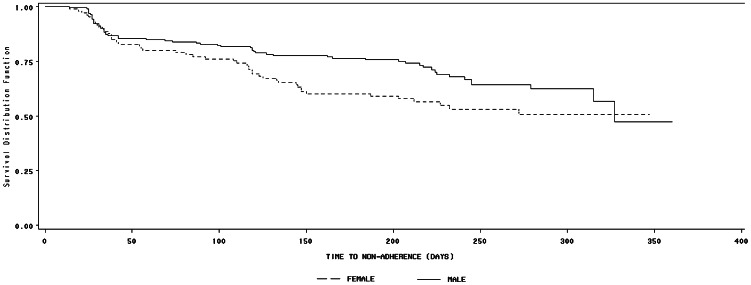
A concurrent prospective study of patients initiating antiretroviral therapy in Brazil was conducted from 2001-2002. The self-reported measurement of adherence was defined as an intake of less than 95% of the prescribed number of doses. Only the first occurrence of non-adherence was considered in this analysis. All analyses were stratified by gender. A Cox proportional hazard model was used to estimate the risk of non-adherence, and the time to non-adherence was estimated using the Kaplan-Meier method.
The cumulative incidence of non-adherence was 34.6% (29.7% and 43.9% among men and women, respectively; p=0.010). Marital status (being married or in stable union; p=0.022), alcohol use in the month prior to the baseline interview (p=0.046), and current tobacco use (p=0.005) increased the risk of non-adherence among female participants only, whereas a self-reported difficulty with the antiretroviral treatment was associated with non-adherence in men only. For both men and women, we found that a longer time between the HIV test and first antiretroviral therapy prescription (p=0.028) also presented an increased risk of non-adherence.
In this cohort study, the incidence of non-adherence was 1.5 times greater among women compared to men. Our results reinforce the need to develop interventions that account for gender differences in public referral centers. Additionally, we emphasize that, to achieve and maintain appropriate adherence levels, it is important to understand the barriers to seeking and utilizing health care services.
本研究旨在确定与首次抗逆转录病毒处方后 12 个月内首次不依从相关的因素中的性别差异。
这是一项 2001-2002 年在巴西开展的同时进行的前瞻性抗逆转录病毒治疗患者研究。通过自我报告的方式测量药物依从性,定义为摄入的处方剂量不足 95%。本分析仅考虑首次不依从的发生情况。所有分析均按性别分层。使用 Cox 比例风险模型估计不依从的风险,使用 Kaplan-Meier 方法估计不依从的时间。
不依从的累积发生率为 34.6%(男性分别为 29.7%和 43.9%,女性为 34.6%;p=0.010)。婚姻状况(已婚或稳定的伴侣关系;p=0.022)、基线访谈前一个月的酒精使用(p=0.046)和当前吸烟(p=0.005)仅增加女性参与者的不依从风险,而自我报告的抗逆转录病毒治疗困难与男性的不依从相关。对于男性和女性,我们发现 HIV 检测与首次抗逆转录病毒治疗处方之间的时间间隔较长(p=0.028)也会增加不依从的风险。
在这项队列研究中,女性的不依从发生率比男性高 1.5 倍。我们的研究结果强调了在公共转诊中心制定考虑到性别差异的干预措施的必要性。此外,我们强调,为了实现并维持适当的依从水平,了解寻求和利用医疗保健服务的障碍非常重要。