Cybulska-Stopa Bożena, Ziobro Marek, Skoczek Marta, Kojs-Pasińska Ewelina, Cedrych Ida, Brandys Anna
Department of Systemic and Generalized Malignancies, Department of Centre of Oncology Maria Sklodowska-Curie Memorial Centre, Krakow, Poland.
Contemp Oncol (Pozn). 2013;17(1):78-82. doi: 10.5114/wo.2013.33779. Epub 2013 Mar 15.
The study examined the response rate, response duration and toxicity of vinorelbine and fluorouracil or vinorelbine alone in pretreated metastatic breast cancer.
Between June 2001 and September 2009, a group of 103 patients with locally advanced or metastatic breast cancer, who had progressed after anthracycline/taxane chemotherapy, was treated with a vinorelbine-based regimen. The treatment consisted of vinorelbine 25 mg/m(2) and 5-fluorouracil (5-FU) 500 mg/m(2) administered intravenously on days 1 and 8 of each cycle (53 patients) or vinorelbine alone at a dose of 30 mg/m(2) on day 1 and 8 of the cycle, every 3 weeks (50 patients). Patients received chemotherapy as a second or further line of therapy. Treatment was continued until disease progression or unacceptable toxicity. The median age of patients treated with vinorelbine with 5FU was 54 years (range 38-76), and 55.5 years (range 38-73) in the group receiving vinorelbine monotherapy. A total of 417 cycles of chemotherapy were administered - 177 cycles of vinorelbine with 5-FU and 137 cycles of vinorelbine monotherapy. Patients were treated for a median of 4 cycles (range: 1 to 11 cycles). The evaluation of treatment effect was possible in 93 patients (10 patients received only one treatment cycle).
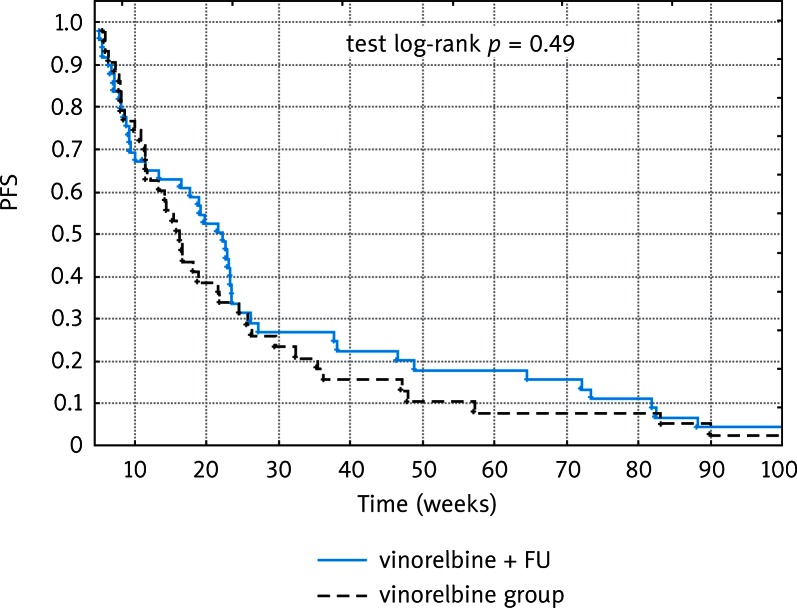
The overall response rate (ORR) was 17% (7), including 2 (4%) complete responses (CR) and 5 (10.5%) partial responses (PR). Stable disease (SD) was observed in 50% of patients receiving vinorelbine with 5-FU (24 patients). In a group receiving vinorelbine alone the ORR was 20% (9), including 9 PR (20%) and 16 SD (35.5%). The median time to progression (TTP) for the entire group was 18 weeks (95% CI), 22 weeks among patients treated with vinorelbine with 5-FU and 16 weeks for a second group. The most common hematologic adverse events were neutropenia (20% of cycles) and thrombocytopenia (4%), with grade 3/4 incidence of 8% and 1.5% [according to National Cancer Institute Common Toxicity Criteria (NCI CTC)]. Nausea and vomiting were the most frequent non-hematologic forms of toxicity, occurring in 13% of cycles. The doses of cytotoxics were reduced in 26 (25%) cases. There were no treatment-related deaths.
Vinorelbine alone or in combination with 5-FU is an effective and safe treatment for pretreated advanced/ metastatic breast cancer patients. The combination of vinorelbine with 5-FU appears to be a more efficacious regimen than vinorelbine alone.
本研究考察了长春瑞滨联合氟尿嘧啶或单独使用长春瑞滨治疗经治转移性乳腺癌的缓解率、缓解持续时间及毒性。
2001年6月至2009年9月,一组103例局部晚期或转移性乳腺癌患者,在蒽环类/紫杉类化疗后病情进展,接受了以长春瑞滨为基础的治疗方案。治疗方案为每个周期的第1天和第8天静脉注射长春瑞滨25mg/m²和5-氟尿嘧啶(5-FU)500mg/m²(53例患者),或每个周期的第1天和第8天单独静脉注射长春瑞滨30mg/m²,每3周一次(50例患者)。患者接受化疗作为二线或更后线治疗。治疗持续至疾病进展或出现不可接受的毒性。接受长春瑞滨联合5-FU治疗的患者中位年龄为54岁(范围38 - 76岁),接受长春瑞滨单药治疗组的中位年龄为55.5岁(范围38 - 73岁)。共进行了417个化疗周期 - 长春瑞滨联合5-FU治疗177个周期,长春瑞滨单药治疗137个周期。患者接受治疗的中位周期数为4个周期(范围:1至11个周期)。93例患者(10例患者仅接受了1个治疗周期)可进行治疗效果评估。
总缓解率(ORR)为17%(7例),包括2例(4%)完全缓解(CR)和5例(10.5%)部分缓解(PR)。接受长春瑞滨联合5-FU治疗的患者中50%(24例)观察到疾病稳定(SD)。在接受长春瑞滨单药治疗的组中,ORR为20%(9例),包括9例PR(20%)和16例SD(35.5%)。整个组的中位疾病进展时间(TTP)为18周(95%CI),长春瑞滨联合5-FU治疗的患者为22周,另一组为16周。最常见的血液学不良事件是中性粒细胞减少(20%的周期)和血小板减少(4%),3/4级发生率分别为8%和1.5%[根据美国国立癌症研究所通用毒性标准(NCI CTC)]。恶心和呕吐是最常见的非血液学毒性形式,发生在13%的周期中。26例(25%)患者降低了细胞毒性药物的剂量。无治疗相关死亡。
长春瑞滨单独或联合5-FU是治疗经治晚期/转移性乳腺癌患者的有效且安全的治疗方法。长春瑞滨联合5-FU似乎比长春瑞滨单药治疗更有效。