Eichler Klaus, Hess Sascha, Chmiel Corinne, Bögli Karin, Sidler Patrick, Senn Oliver, Rosemann Thomas, Brügger Urs
Winterthur Institute of Health Economics, Zurich University of Applied Sciences, Winterthur, Switzerland.
City Hospital Waid, Zurich, Switzerland Institute of General Practice and Health Services Research, University of Zurich, Zurich, Switzerland.
Emerg Med J. 2014 Oct;31(10):818-23. doi: 10.1136/emermed-2013-202760. Epub 2013 Jul 12.
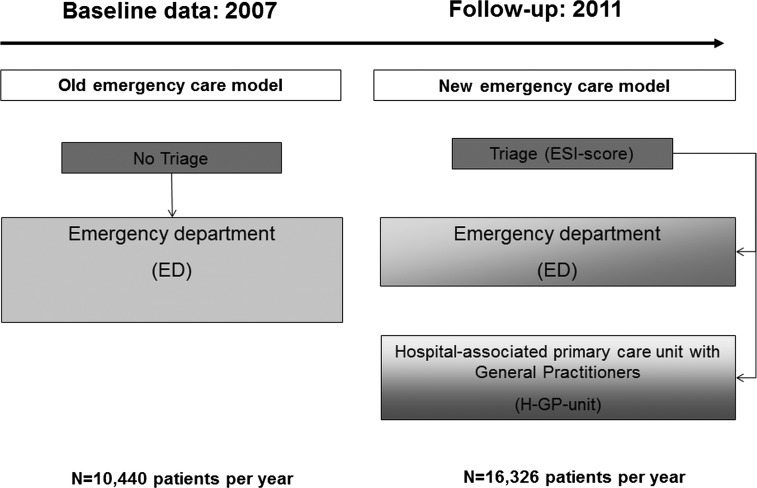
Emergency departments (EDs) are increasingly overcrowded by walk-in patients. However, little is known about health-economic consequences resulting from long waiting times and inefficient use of specialised resources. We have evaluated a quality improvement project of a Swiss urban hospital: In 2009, a triage system and a hospital-associated primary care unit with General Practitioners (H-GP-unit) were implemented beside the conventional hospital ED. This resulted in improved medical service provision with reduced process times and more efficient diagnostic testing. We now report on health-economic effects.
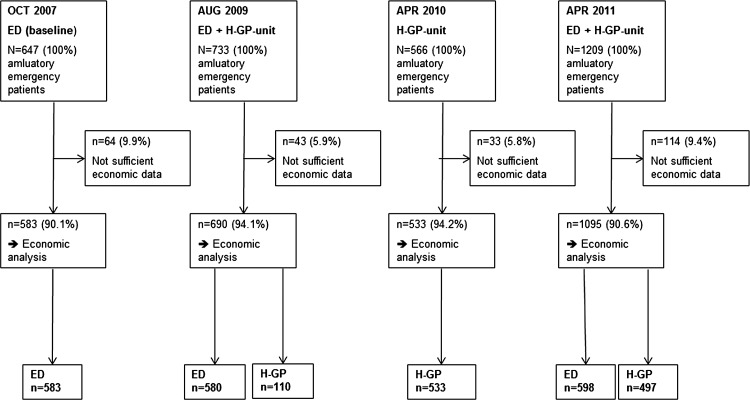
From the hospital perspective, we performed a cost comparison study analysing treatment costs in the old emergency model (ED, only) versus treatment costs in the new emergency model (triage plus ED plus H-GP-unit) from 2007 to 2011. Hospital cost accounting data were applied. All consecutive outpatient emergency contacts were included for 1 month in each follow-up year.
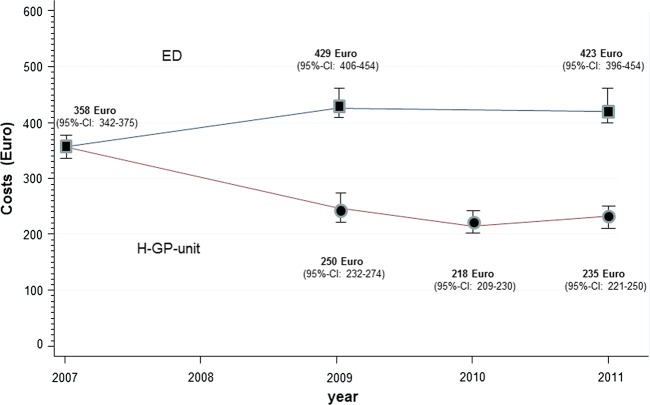
The annual number of outpatient emergency contacts increased from n=10 440 (2007; baseline) to n=16 326 (2011; after intervention), reflecting a general trend. In 2007, mean treatment costs per outpatient were €358 (95% CI 342 to 375). Until 2011, costs increased in the ED (€423 (396 to 454)), but considerably decreased in the H-GP-unit (€235 (221 to 250)). Compared with 2007, the annual local budget spent for treatment of 16 326 patients in 2011 showed cost reductions of €417 600 (27 200 to 493 600) after adjustment for increasing patient numbers.
From the health-economic point of view, our new service model shows 'dominance' over the old model: While quality of service provision improved (reduced waiting times; more efficient resource use in the H-GP-unit), treatment costs sustainably decreased against the secular trend of increase.
急诊科(ED)中自行前来就诊的患者日益增多,导致人满为患。然而,对于长时间等待和专业资源利用效率低下所带来的健康经济后果,我们却知之甚少。我们评估了一家瑞士城市医院的质量改进项目:2009年,在传统医院急诊科之外实施了分诊系统以及设有全科医生的医院附属初级保健单元(H-GP单元)。这使得医疗服务得到改善,流程时间缩短,诊断测试更加高效。我们现在报告其健康经济效应。
从医院角度出发,我们进行了一项成本比较研究,分析了2007年至2011年旧的急诊模式(仅急诊科)与新的急诊模式(分诊 + 急诊科 + H-GP单元)下的治疗成本。应用了医院成本核算数据。在每个随访年份中,连续纳入1个月内所有门诊急诊就诊病例。
门诊急诊就诊的年度数量从2007年的n = 10440(基线)增加到2011年的n = 16326(干预后),呈现出总体上升趋势。2007年,每位门诊患者的平均治疗成本为358欧元(95%可信区间342至375)。到2011年,急诊科成本有所增加(423欧元(396至454)),但H-GP单元成本大幅下降(235欧元(221至250))。与2007年相比,在对增加的患者数量进行调整后,2011年用于治疗16326名患者的年度地方预算成本降低了417600欧元(27200至493600)。
从健康经济角度来看,我们的新服务模式相对于旧模式显示出“优势”:在服务质量得到改善(等待时间缩短;H-GP单元资源利用更高效)的同时,治疗成本却逆势持续下降。