Division of Population Health Sciences, Medical Research Institute, University of Dundee, Dundee, UK.
BMJ Open. 2013 Jul 16;3(7). doi: 10.1136/bmjopen-2013-003121. Print 2013.
To measure the incidence of Bell's palsy and determine the impact of clinical trial findings on Bell's palsy management in the UK.
Interrupted time series regression analysis and incidence measures.
General practices in the UK contributing to the Clinical Practice Research Datalink (CPRD).
Patients ≥16 years with a diagnosis of Bell's palsy between 2001 and 2012.
(1) Publication of the 2004 Cochrane reviews of clinical trials on corticosteroids and antivirals for Bell's palsy, which made no clear recommendation on their use and (2) publication of the 2007 Scottish Bell's Palsy Study (SBPS), which made a clear recommendation that treatment with prednisolone alone improves chances for complete recovery.
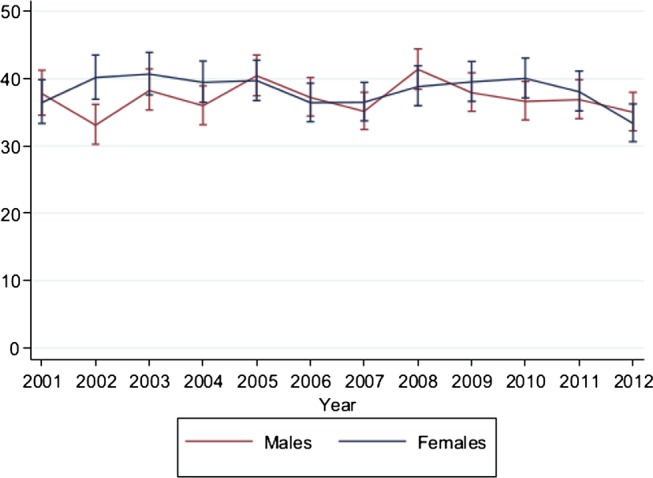
Incidence of Bell's palsy per 100 000 person-years. Changes in the management of Bell's palsy with either prednisolone therapy, antiviral therapy, combination therapy (prednisolone with antiviral therapy) or untreated cases.
During the 12-year period, 14 460 cases of Bell's palsy were identified with an overall incidence of 37.7/100 000 person-years. The 2004 Cochrane reviews were associated with immediate falls in prednisolone therapy (-6.3% (-11.0 to -1.6)), rising trends in combination therapy (1.1% per quarter (0.5 to 1.7)) and falling trends for untreated cases (-0.8% per quarter (-1.4 to -0.3)). SBPS was associated with immediate increases in prednisolone therapy (5.1% (0.9 to 9.3)) and rising trends in prednisolone therapy (0.7% per quarter (0.4 to 1.2)); falling trends in combination therapy (-1.7% per quarter (-2.2 to -1.3)); and rising trends for untreated cases (1.2% per quarter (0.8 to 1.6)). Despite improvements, 44% still remain untreated.
SBPS was clearly associated with change in management, but a significant proportion of patients failed to receive effective treatment, which cannot be fully explained. Clarity and uncertainty in clinical trial recommendations may change clinical practice. However, better ways are needed to understand and circumvent barriers in implementing clinical trial findings.
测量贝尔麻痹的发病率,并确定临床试验结果对英国贝尔麻痹治疗的影响。
中断时间序列回归分析和发病率测量。
为临床实践研究数据链接(CPRD)提供数据的英国普通实践。
2001 年至 2012 年间患有贝尔麻痹的年龄≥16 岁的患者。
(1)发表 2004 年关于皮质类固醇和抗病毒药物治疗贝尔麻痹的 Cochrane 临床试验的评论,该评论未明确推荐使用皮质类固醇和抗病毒药物,(2)发表 2007 年苏格兰贝尔麻痹研究(SBPS),明确建议单独使用泼尼松龙治疗可提高完全康复的机会。
每 100000 人年的贝尔麻痹发病率。用泼尼松龙治疗、抗病毒治疗、联合治疗(泼尼松龙联合抗病毒治疗)或未治疗病例治疗贝尔麻痹的治疗方式的变化。
在 12 年期间,共发现 14460 例贝尔麻痹病例,总发病率为 37.7/100000 人年。2004 年的 Cochrane 评论与泼尼松龙治疗的立即下降有关(-6.3%(-11.0 至-1.6)),联合治疗的上升趋势(每季度 1.1%(0.5 至 1.7))和未治疗病例的下降趋势(每季度-0.8%(-1.4 至-0.3))。SBPS 与泼尼松龙治疗的立即增加有关(5.1%(0.9 至 9.3))和泼尼松龙治疗的上升趋势(每季度 0.7%(0.4 至 1.2));联合治疗的下降趋势(每季度-1.7%(-2.2 至-1.3));未治疗病例的上升趋势(每季度 1.2%(0.8 至 1.6))。尽管有所改善,但仍有 44%的患者未得到有效治疗。
SBPS 与治疗方法的改变明显相关,但仍有相当一部分患者未接受有效治疗,这不能完全解释。临床试验建议的明确性和不确定性可能会改变临床实践。然而,需要更好的方法来理解和规避实施临床试验结果的障碍。