Kiewiet Jordy J S, van Ruler Oddeke, Boermeester Marja A, Reitsma Johannes B
Department of Surgery, Academic Medical Center, Meibergdreef 9, Amsterdam 1105 AZ, The Netherlands.
BMC Surg. 2013 Jul 19;13:28. doi: 10.1186/1471-2482-13-28.
Accurate and timely identification of patients in need of a relaparotomy is challenging since there are no readily available strongholds. The aim of this study is to develop a prediction model to aid the decision-making process in whom to perform a relaparotomy.
Data from a randomized trial comparing surgical strategies for relaparotomy were used. Variables were selected based on previous reports and common clinical sense and screened in a univariable regression analysis to identify those associated with the need for relaparotomy. Variables with the strongest association were considered for the prediction model which was constructed after backward elimination in a multivariable regression analysis. The discriminatory capacity of the model was expressed with the area under the curve (AUC). A cut-off analysis was performed to illustrate the consequences in clinical practice.
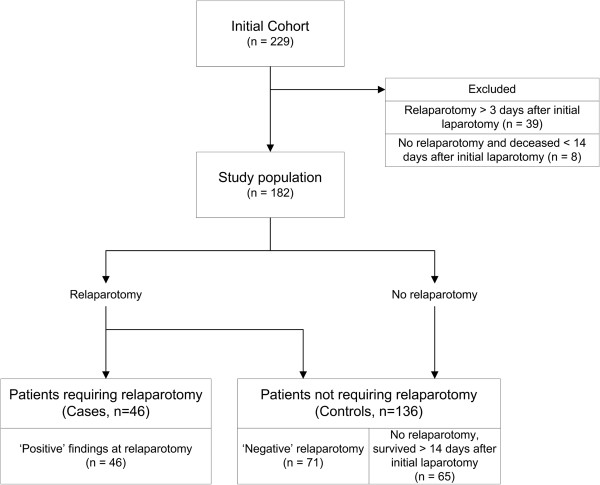
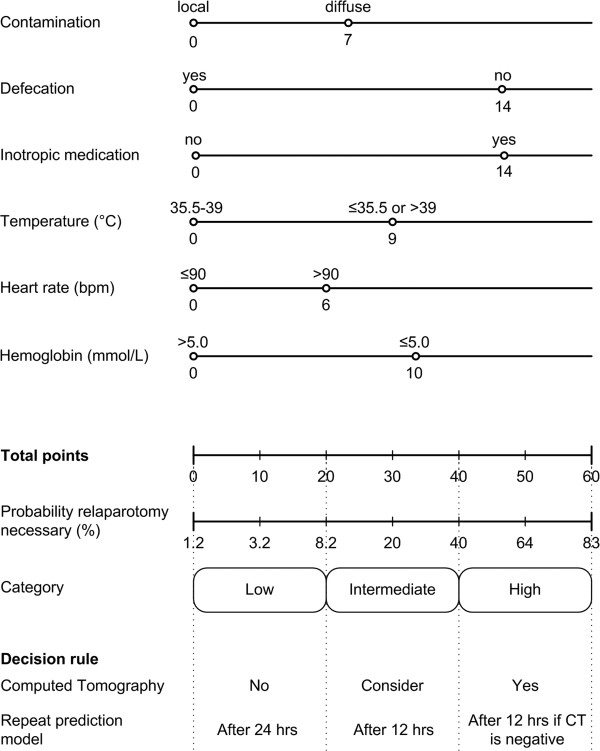
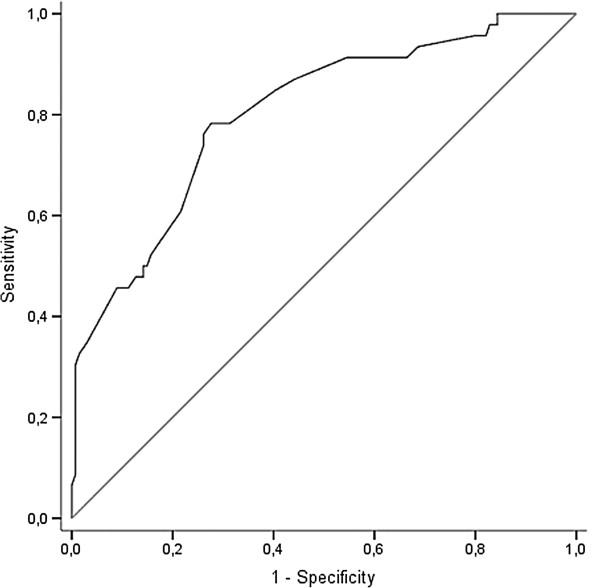
One hundred and eighty-two patients were included; 46 were considered cases requiring a relaparotomy. A prediction model was build containing 6 variables. This final model had an AUC of 0.80 indicating good discriminatory capacity. However, acceptable sensitivity would require a low threshold for relaparotomy leading to an unacceptable rate of negative relaparotomies (63%). Therefore, the prediction model was incorporated in a decision rule were the interval until re-assessment and the use of Computed Tomography are related to the outcome of the model.
To construct a prediction model that will provide a definite answer whether or not to perform a relaparotomy seems a utopia. However, our prediction model can be used to stratify patients on their underlying risk and could guide further monitoring of patients with abdominal sepsis in order to identify patients with suspected ongoing peritonitis in a timely fashion.
由于缺乏现成的可靠依据,准确及时地识别需要再次剖腹手术的患者具有挑战性。本研究的目的是开发一种预测模型,以辅助决定对哪些患者进行再次剖腹手术。
使用一项比较再次剖腹手术手术策略的随机试验数据。根据先前的报告和一般临床常识选择变量,并在单变量回归分析中进行筛选,以确定那些与再次剖腹手术需求相关的变量。在多变量回归分析中通过向后消除法构建预测模型时,考虑关联性最强的变量。模型的鉴别能力用曲线下面积(AUC)表示。进行了截断分析以说明在临床实践中的后果。
纳入了182例患者;46例被视为需要再次剖腹手术的病例。构建了一个包含6个变量的预测模型。该最终模型的AUC为0.80,表明具有良好的鉴别能力。然而,要获得可接受的敏感性,需要对再次剖腹手术设定较低的阈值,这会导致不可接受的阴性再次剖腹手术率(63%)。因此,将预测模型纳入了一个决策规则,其中再次评估的间隔时间和计算机断层扫描的使用与模型的结果相关。
构建一个能明确回答是否进行再次剖腹手术的预测模型似乎是不切实际的。然而,我们的预测模型可用于根据患者的潜在风险进行分层,并可指导对腹部脓毒症患者的进一步监测,以便及时识别疑似持续性腹膜炎的患者。