Department of Surgery, St. Jude Children's Research Hospital, Memphis, TN, USA.
J Pediatr Surg. 2013 Jul;48(7):1598-603. doi: 10.1016/j.jpedsurg.2013.04.019.
To determine whether performing adrenalectomy at the time of nephrectomy for unilateral Wilms tumor impacts clinical outcome.
We reviewed information on all patients enrolled on National Wilms Tumor Study-4 and -5. Data were abstracted on patient demographics, tumor characteristics, surgical and pathologic status of the adrenal gland, and patient outcomes. The primary endpoints were intraoperative spill and five-year event-free survival (EFS) in patients who did or did not undergo adrenalectomy.
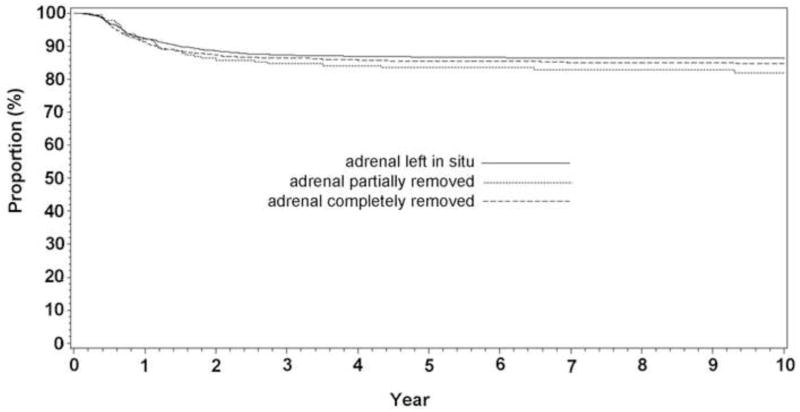
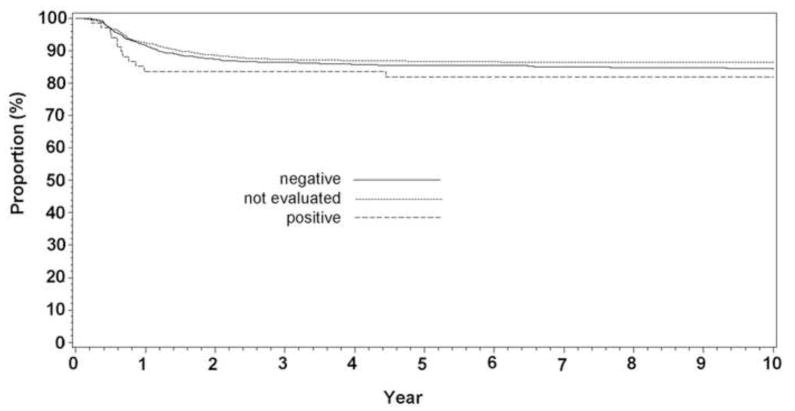
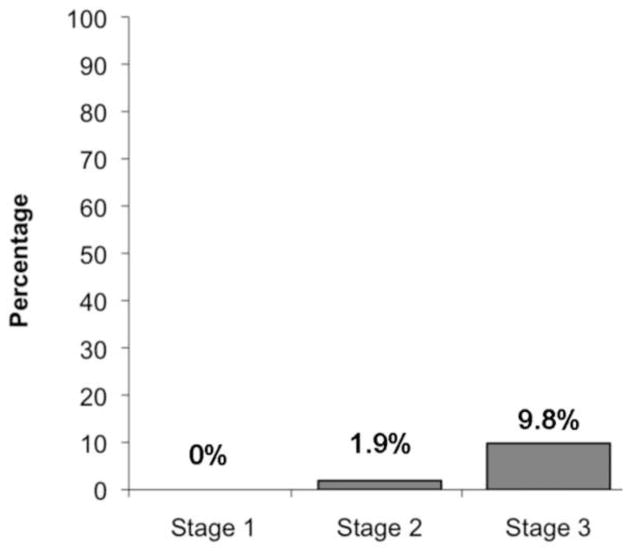
Of 3825 patients with complete evaluable data, the adrenal was left in situ in 2264 (57.9%) patients, and was removed completely in 1367 patients (36.7%) or partially in 194 patients (5.2%). Of the adrenal glands removed, 68 (4.4%) contained tumor. Adrenal involvement was more common in patients with stage 3 (9.8%) than stage 2 disease (1.9%; p < 0.0001). After controlling for stage and histopathology, five-year EFS was similar whether or not the adrenal gland was removed (p = 0.48), or involved with tumor (p = 0.81); however, intraoperative spill rates were higher in patients undergoing adrenalectomy (26.1% vs 15.5%, p < 0.0001), likely due to larger tumor size or technical factors. No patient had clinical evidence of adrenal insufficiency or tumor recurrence in the adrenal gland during follow-up (median 9.9 years).
Sparing the adrenal gland during nephrectomy for unilateral Wilms tumor was not associated with a higher incidence of intraoperative spill and was associated with a similar oncologic outcome, on a per-stage basis, with cases where the adrenal was removed. Thus, adrenalectomy should not be considered mandatory during radical nephrectomy for Wilms tumor.
确定单侧肾母细胞瘤行肾切除术时是否行肾上腺切除术对临床结果的影响。
我们回顾了参加国家肾母细胞瘤研究 4 期和 5 期的所有患者的信息。提取了患者人口统计学、肿瘤特征、肾上腺的手术和病理状态以及患者结局的数据。主要终点是行或不行肾上腺切除术的患者术中肿瘤溢出和 5 年无事件生存率(EFS)。
在 3825 例具有完整可评估数据的患者中,2264 例(57.9%)患者的肾上腺保留原位,1367 例(36.7%)或 194 例(5.2%)患者完全切除,194 例(5.2%)患者部分切除。在切除的肾上腺中,有 68 例(4.4%)含有肿瘤。肾上腺受累在 3 期(9.8%)患者中比 2 期(1.9%;p < 0.0001)更常见。在控制分期和组织病理学后,无论是否切除肾上腺,5 年 EFS 相似(p = 0.48),或肿瘤累及肾上腺(p = 0.81);然而,行肾上腺切除术的患者术中肿瘤溢出率更高(26.1%比 15.5%,p < 0.0001),可能是由于肿瘤较大或技术因素。在随访期间(中位数为 9.9 年),没有患者出现肾上腺功能不全或肾上腺肿瘤复发的临床证据。
单侧肾母细胞瘤行肾切除术时保留肾上腺与术中肿瘤溢出发生率较高无关,且在各分期情况下,与切除肾上腺的病例具有相似的肿瘤学结局。因此,在肾母细胞瘤根治性肾切除术中,不应该将肾上腺切除术视为强制性手术。