JAMA Pediatr. 2013 Sep;167(9):851-8. doi: 10.1001/jamapediatrics.2013.186.
Community-acquired pneumonia (CAP) remains one of the most common indications for pediatric hospitalization in the United States, and it is frequently the focus of research and quality studies. Use of administrative data is increasingly common for these purposes, although proper validation is required to ensure valid study conclusions.
To validate administrative billing data for hospitalizations owing to childhood CAP.
Case-control study of 4 tertiary care, freestanding children’s hospitals in the United States.
A total of 998 medical records of a 25% random sample of 3646 children discharged in 2010 with at least 1 International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code representing possible pneumonia were reviewed. Discharges (matched on date of admission) without a pneumonia-related discharge code were also examined to identify potential missed pneumonia cases. Two reference standards, based on provider diagnosis alone (provider confirmed) or in combination with consistent clinical and radiographic evidence of pneumonia (definite), were used to identify CAP.
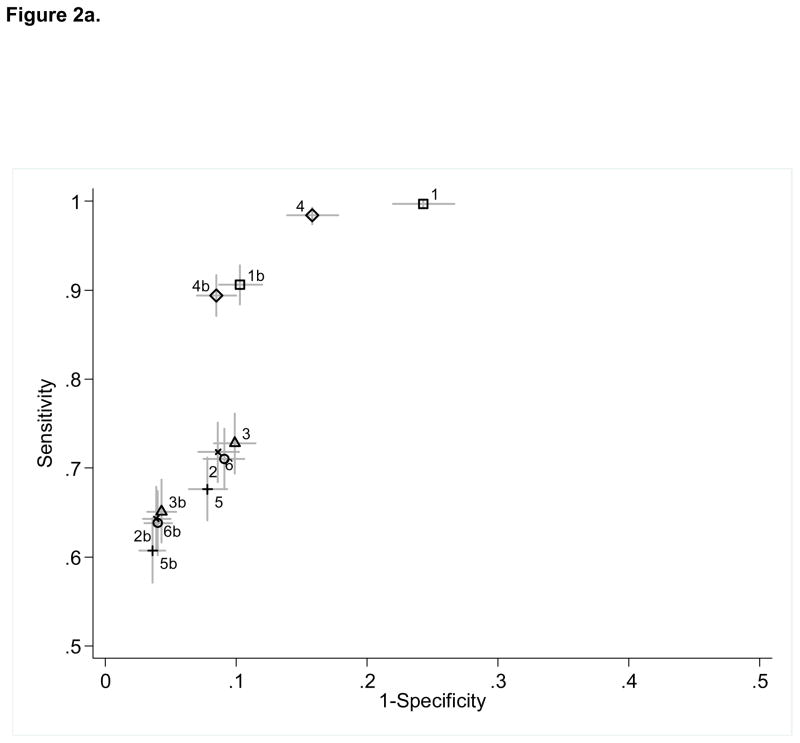
Twelve ICD-9-CM–based coding strategies, each using a combination of primary or secondary codes representing pneumonia or pneumonia-related complications. Six algorithms excluded children with complex chronic conditions.
Sensitivity, specificity, and negative and positive predictive values (NPV and PPV, respectively) of the 12 identification strategies.
For provider-confirmed CAP (n = 680), sensitivity ranged from 60.7% to 99.7%; specificity, 75.7% to 96.4%; PPV, 67.9% to 89.6%; and NPV, 82.6% to 99.8%. For definite CAP (n = 547), sensitivity ranged from 65.6% to 99.6%; specificity, 68.7% to 93.0%; PPV, 54.6% to 77.9%; and NPV, 87.8% to 99.8%. Unrestricted use of the pneumonia-related codes was inaccurate, although several strategies improved specificity to more than 90% with a variable effect on sensitivity. Excluding children with complex chronic conditions demonstrated the most favorable performance characteristics. Performance of the algorithms was similar across institutions.
Administrative data are valuable for studying pediatric CAP hospitalizations. The strategies presented here will aid in the accurate identification of relevant and comparable patient populations for research and performance improvement studies.
在美国,社区获得性肺炎(CAP)仍然是小儿住院的最常见原因之一,它也是研究和质量研究的重点。尽管需要进行适当的验证以确保研究结论的有效性,但越来越多的人使用行政数据来实现这些目的。
验证因儿童 CAP 而住院的行政计费数据。
美国四家三级保健、独立儿童医院的病例对照研究。
对 2010 年至少有一个代表可能肺炎的国际疾病分类,第 9 版,临床修正(ICD-9-CM)代码的 3646 名出院儿童的 25%随机样本的 998 份医疗记录进行了回顾。还检查了没有肺炎相关出院代码的出院情况,以确定潜在的漏报肺炎病例。使用两个参考标准,仅基于提供者诊断(提供者确认)或结合一致的临床和放射影像学肺炎证据(明确),来识别 CAP。
12 种基于 ICD-9-CM 的编码策略,每种策略都使用代表肺炎或肺炎相关并发症的主要或次要代码的组合。六个算法排除了患有复杂慢性疾病的儿童。
12 种识别策略的敏感性、特异性、阴性和阳性预测值(NPV 和 PPV)。
对于提供者确认的 CAP(n=680),敏感性范围为 60.7%至 99.7%;特异性为 75.7%至 96.4%;PPV 为 67.9%至 89.6%;NPV 为 82.6%至 99.8%。对于明确的 CAP(n=547),敏感性范围为 65.6%至 99.6%;特异性为 68.7%至 93.0%;PPV 为 54.6%至 77.9%;NPV 为 87.8%至 99.8%。尽管使用肺炎相关代码的无限制使用并不准确,但有几种策略可以将特异性提高到 90%以上,同时对敏感性产生不同的影响。排除患有复杂慢性疾病的儿童表现出最有利的性能特征。这些算法在各机构的表现相似。
行政数据对于研究儿科 CAP 住院治疗很有价值。本文提出的策略将有助于准确识别相关且可比的患者群体,以进行研究和绩效改进研究。