Smolen Josef S, Kay Jonathan, Matteson Eric L, Landewé Robert, Hsia Elizabeth C, Xu Stephen, Zhou Yiying, Doyle Mittie K
Division of Rheumatology, Department of Medicine III, Medical University of Vienna, and 2nd Department of Medicine, Hietzing Hospital, Vienna, Austria.
Division of Rheumatology, Department of Medicine, University of Massachusetts Medical School and UMass Memorial Medical Center, Worcester, Massachusetts, USA.
Ann Rheum Dis. 2014 Oct;73(10):1811-8. doi: 10.1136/annrheumdis-2013-203435. Epub 2013 Jul 29.
Evaluate golimumab in patients with active rheumatoid arthritis (RA) and previous tumour necrosis factor-α (TNF) inhibitor use.
Patients (n=461) previously receiving ≥1 TNF inhibitor were randomised to subcutaneous injections of placebo, golimumab 50 mg or golimumab 100 mg q4 weeks. Primary endpoint (≥20% improvement in American College of Rheumatology (ACR20) criteria at week 14) findings have been reported for all patients in the trial. Reported herein are further assessments of efficacy/safety among patients receiving golimumab+methotrexate (MTX).
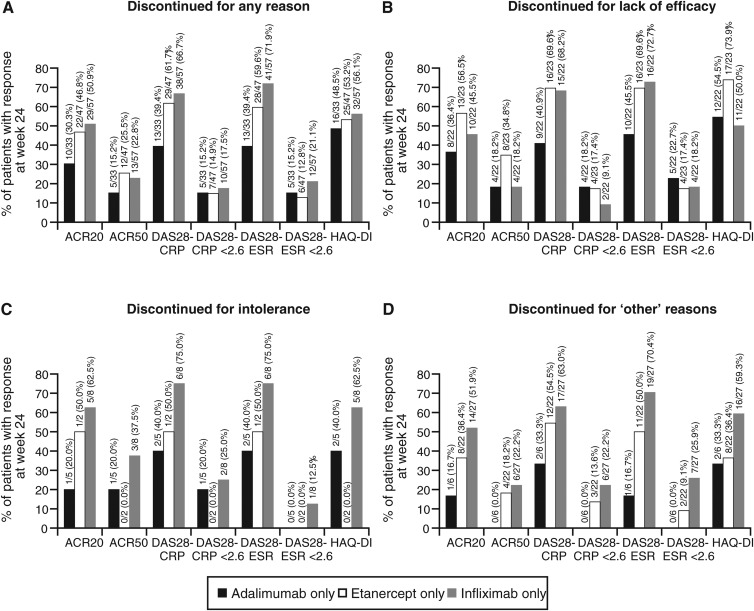
Among efficacy-evaluable patients who received MTX at baseline, more receiving golimumab+MTX (n=201) than placebo+MTX (n=103) achieved ACR20 (40.8% vs 14.6%), ACR50 (20.9% vs 3.9%), and ACR70 (11.4% vs 2.9%) responses at week 24. Among the 137 patients who had received only one prior TNF inhibitor (adalimumab, n=33; etanercept, n=47; and infliximab, n=57), week 24 ACR20 rates were 30.3%, 46.8% and 50.9%, respectively, and thus lowest among those who previously used adalimumab. ACR20 response rates were 44.5% (61/137), 36.2% (17/47) and 23.5% (4/17) among patients who had received one, two or three TNF inhibitors, respectively. Adverse event (AE) rates were comparable across type/number of prior anti-TNF agents, but appeared somewhat higher among patients who discontinued previous TNF inhibitor(s) due to intolerance (37/49, 75.5%) versus lack of efficacy (LOE, 113/191, 59.2%).
Patients with active RA previously treated with ≥1 TNF inhibitor had clinically relevant improvement with golimumab+MTX, which appeared somewhat enhanced among those who received only etanercept or infliximab as their prior TNF inhibitor. Golimumab+MTX safety appeared similar across patients, regardless of TNF inhibitor(s) previously used, with fewer AEs occurring among patients who discontinued prior therapy for LOE.
评估戈利木单抗在患有活动性类风湿关节炎(RA)且既往使用过肿瘤坏死因子-α(TNF)抑制剂的患者中的疗效。
既往接受过≥1种TNF抑制剂治疗的患者(n = 461)被随机分为皮下注射安慰剂、每4周注射50 mg戈利木单抗或每4周注射100 mg戈利木单抗。该试验中所有患者的主要终点(第14周时美国风湿病学会(ACR20)标准改善≥20%)结果已报告。本文报告的是接受戈利木单抗+甲氨蝶呤(MTX)治疗的患者的疗效/安全性的进一步评估。
在基线时接受MTX治疗的可评估疗效的患者中,接受戈利木单抗+MTX(n = 201)的患者在第24周达到ACR20(40.8%对14.6%)、ACR50(20.9%对3.9%)和ACR70(11.4%对2.9%)反应的人数多于接受安慰剂+MTX(n = 103)的患者。在仅接受过一种既往TNF抑制剂(阿达木单抗,n = 33;依那西普,n = 47;英夫利昔单抗,n = 57)治疗的137例患者中,第24周的ACR20率分别为30.3%、46.8%和50.9%,因此在既往使用阿达木单抗的患者中最低。在接受过一种、两种或三种TNF抑制剂治疗的患者中,ACR20反应率分别为44.5%(61/137)、36.2%(17/47)和23.5%(4/17)。不良事件(AE)发生率在既往抗TNF药物的类型/数量方面相当,但因不耐受而停用既往TNF抑制剂的患者(37/49,75.5%)的AE发生率似乎略高于因疗效不佳(LOE,113/191,59.2%)而停用的患者。
既往接受过≥1种TNF抑制剂治疗的活动性RA患者使用戈利木单抗+MTX有临床相关改善,在仅接受依那西普或英夫利昔单抗作为既往TNF抑制剂的患者中改善似乎有所增强。无论既往使用何种TNF抑制剂,戈利木单抗+MTX的安全性在患者中似乎相似,因疗效不佳而停用既往治疗的患者发生的AE较少。