CRI New England, Harvard Medical School, Boston, Massachusetts, USA.
BMJ Open. 2013 Aug 1;3(8):e003028. doi: 10.1136/bmjopen-2013-003028.
Lower pill burden leads to improved antiretroviral therapy (ART) adherence among HIV patients. Simpler dosing regimens have not been widely explored in real-world populations. We retrospectively assessed ART adherence, all-cause hospitalisation risk and costs, and other healthcare utilisation and costs in Medicaid enrollees with HIV treated with ART as a once-daily single-tablet regimen (STR) or two or more pills per day (2+PPD).
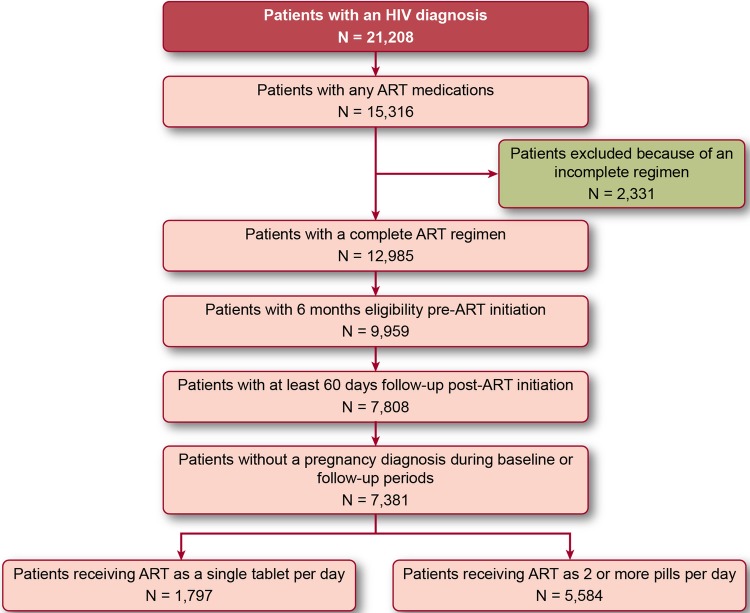
Patients with an HIV diagnosis from 2005 to 2009 receiving complete ART (ie, two nucleoside/nucleotide reverse transcriptase inhibitors plus a third agent) for ≥60 days as STR or 2+PPD were selected and followed until the first of (1) discontinuation of the complete ART, (2) loss of enrolment or (3) end of database. Adherence was measured using the medication possession ratio. Monthly all-cause healthcare utilisation and costs were observed from regimen initiation until follow-up end.
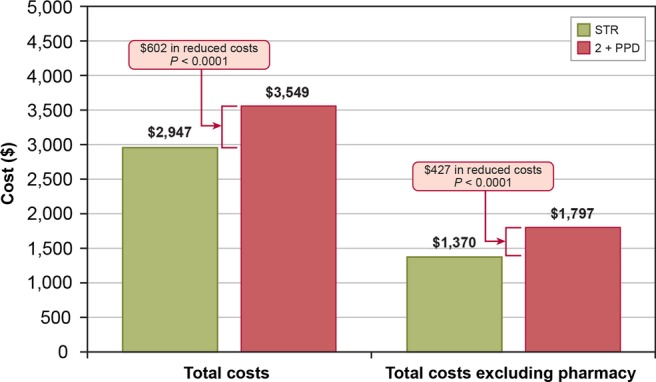
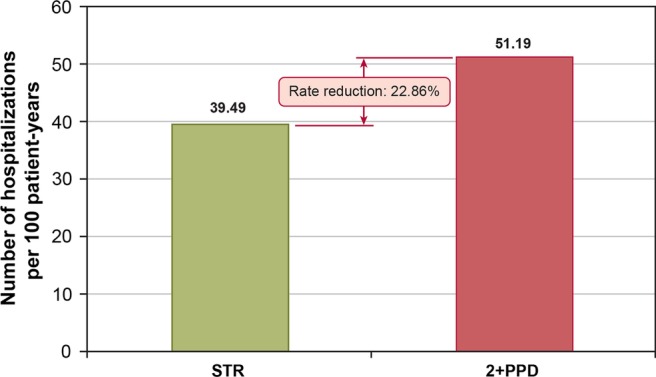
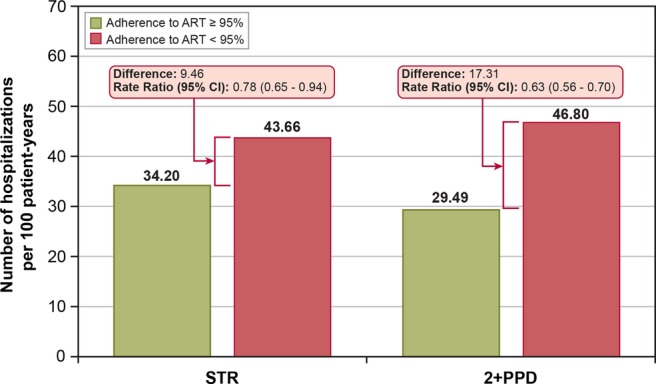
Of the 7381 patients who met inclusion criteria, 1797 were treated with STR and 5584 with 2+PPD. STR patients were significantly more likely to reach 95% adherence and had fewer hospitalisations than 2+PPD patients (both p<0.01). STR patients had mean (SD) total monthly costs of $2959 ($4962); 2+PPD patients had $3544 ($5811; p<0.001). Hospital costs accounted for 53.8% and pharmacy costs accounted for 32.5% of this difference. Multivariate analyses found that STR led to a 23% reduction in hospitalisations and a 17% reduction in overall healthcare costs. ART adherence appears to be a key mechanism mediating hospitalisation risk, as patients with ≥95% adherence (regardless of regimen type) had a lower hospitalisation rate compared with <95% adherence.
While it was expected that STR patients would have lower pharmacy costs, we also found that STR patients had fewer hospitalisations and lower hospital costs than 2+PPD patients, resulting in significantly lower total healthcare costs for STR patients.
降低药物负担可提高 HIV 患者接受抗逆转录病毒治疗(ART)的依从性。简化的给药方案在真实世界人群中尚未得到广泛探索。我们回顾性评估了医疗保险(Medicaid)患者接受 ART 治疗时的 ART 依从性、全因住院风险和费用,以及其他医疗保健利用和成本,这些患者的 HIV 诊断为 2005 年至 2009 年,接受至少 60 天的每日一次单片方案(STR)或每日两片或以上(2+PPD)的 ART 治疗。
选择了接受 STR 或 2+PPD 治疗的至少接受 60 天完整 ART(即两种核苷/核苷酸逆转录酶抑制剂加第三种药物)的 HIV 诊断患者,并随访至以下三种情况之一发生:(1)完整 ART 停药;(2)失去参保资格;(3)数据库结束。使用药物占有比来衡量依从性。从方案开始到随访结束,观察每月的全因医疗保健利用和成本。
在符合纳入标准的 7381 名患者中,1797 名接受 STR 治疗,5584 名接受 2+PPD 治疗。STR 患者达到 95%依从性的可能性明显高于 2+PPD 患者(均 P<0.01),且住院率也低于 2+PPD 患者(均 P<0.01)。STR 患者的平均(SD)每月总费用为 2959 美元(4962 美元);2+PPD 患者为 3544 美元(5811 美元;P<0.001)。住院费用占此差异的 53.8%,而药品费用占 32.5%。多变量分析发现,STR 可使住院率降低 23%,总医疗保健费用降低 17%。ART 依从性似乎是调节住院风险的关键机制,因为依从性≥95%(无论方案类型如何)的患者与依从性<95%的患者相比,住院率更低。
虽然预计 STR 患者的药品费用会更低,但我们还发现,与 2+PPD 患者相比,STR 患者的住院次数和住院费用更低,因此 STR 患者的总医疗保健费用显著更低。