Luyckx Valerie A, Shukha Khuloud, Brenner Barry M
Associate Professor, Division of Nephrology, University of Alberta, Edmonton, Alberta, Canada;
Rambam Maimonides Med J. 2011 Oct 31;2(4):e0061. doi: 10.5041/RMMJ.10061. Print 2011 Oct.
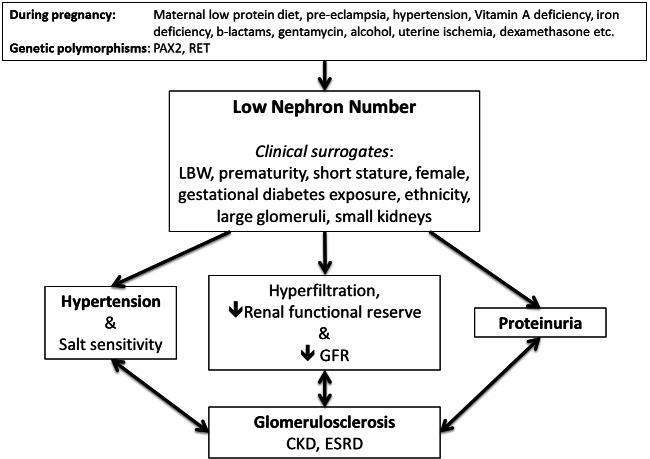
Epidemiologic studies now strongly support the hypothesis, proposed over two decades ago, that developmental programming of the kidney impacts an individual's risk for hypertension and renal disease in later life. Low birth weight is the strongest current clinical surrogate marker for an adverse intrauterine environment and, based on animal and human studies, is associated with a low nephron number. Other clinical correlates of low nephron number include female gender, short adult stature, small kidney size, and prematurity. Low nephron number in Caucasian and Australian Aboriginal subjects has been shown to be associated with higher blood pressures, and, conversely, hypertension is less prevalent in individuals with higher nephron numbers. In addition to nephron number, other programmed factors associated with the increased risk of hypertension include salt sensitivity, altered expression of renal sodium transporters, altered vascular reactivity, and sympathetic nervous system overactivity. Glomerular volume is universally found to vary inversely with nephron number, suggesting a degree of compensatory hypertrophy and hyperfunction in the setting of a low nephron number. This adaptation may become overwhelmed in the setting of superimposed renal insults, e.g. diabetes mellitus or rapid catch-up growth, leading to the vicious cycle of on-going hyperfiltration, proteinuria, nephron loss and progressive renal functional decline. Many millions of babies are born with low birth weight every year, and hypertension and renal disease prevalences are increasing around the globe. At present, little can be done clinically to augment nephron number; therefore adequate prenatal care and careful postnatal nutrition are crucial to optimize an individual's nephron number during development and potentially to stem the tide of the growing cardiovascular and renal disease epidemics worldwide.
流行病学研究如今有力地支持了二十多年前提出的假说,即肾脏的发育编程会影响个体在晚年患高血压和肾病的风险。低出生体重是当前不良子宫内环境最强的临床替代标志物,基于动物和人体研究,它与肾单位数量减少有关。肾单位数量减少的其他临床相关因素包括女性性别、成年后身材矮小、肾脏体积小和早产。在白种人和澳大利亚原住民中,肾单位数量减少已被证明与血压升高有关,相反,肾单位数量较多的个体中高血压患病率较低。除了肾单位数量外,与高血压风险增加相关的其他编程因素还包括盐敏感性、肾钠转运体表达改变、血管反应性改变和交感神经系统活动过度。普遍发现肾小球体积与肾单位数量呈反比,这表明在肾单位数量较少的情况下存在一定程度的代偿性肥大和功能亢进。在叠加肾脏损伤的情况下,如糖尿病或快速追赶生长,这种适应可能会不堪重负,导致持续的超滤、蛋白尿、肾单位丢失和肾功能进行性下降的恶性循环。每年有数以百万计的低出生体重儿出生,全球高血压和肾病的患病率正在上升。目前,临床上几乎无法增加肾单位数量;因此,充分的产前护理和精心的产后营养对于在发育过程中优化个体的肾单位数量以及潜在地阻止全球心血管和肾病流行趋势至关重要。