Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, Texas.
Am J Hematol. 2013 Dec;88(12):1024-9. doi: 10.1002/ajh.23560. Epub 2013 Sep 12.
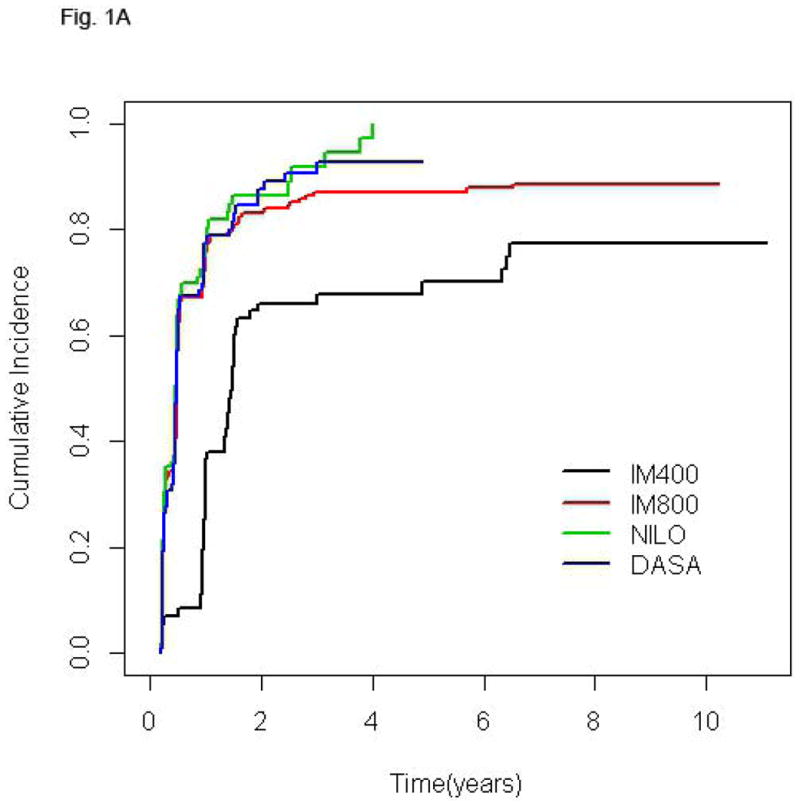
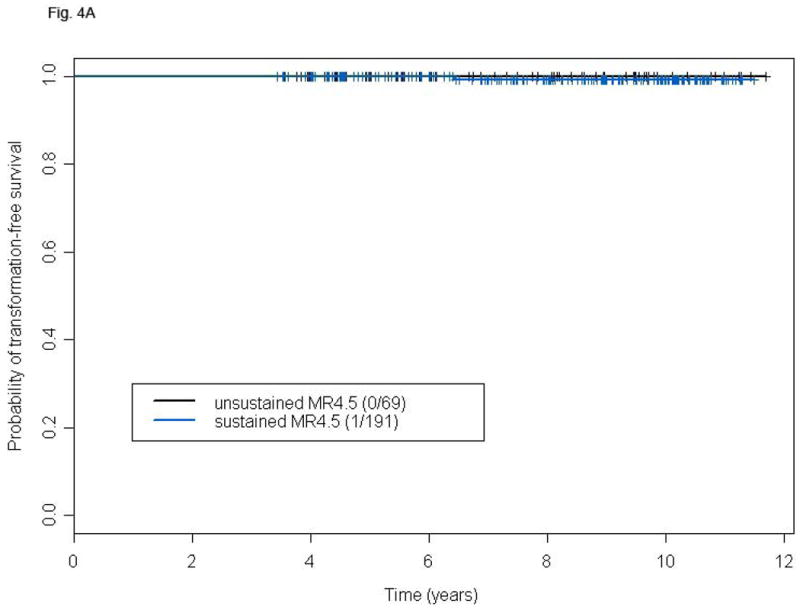
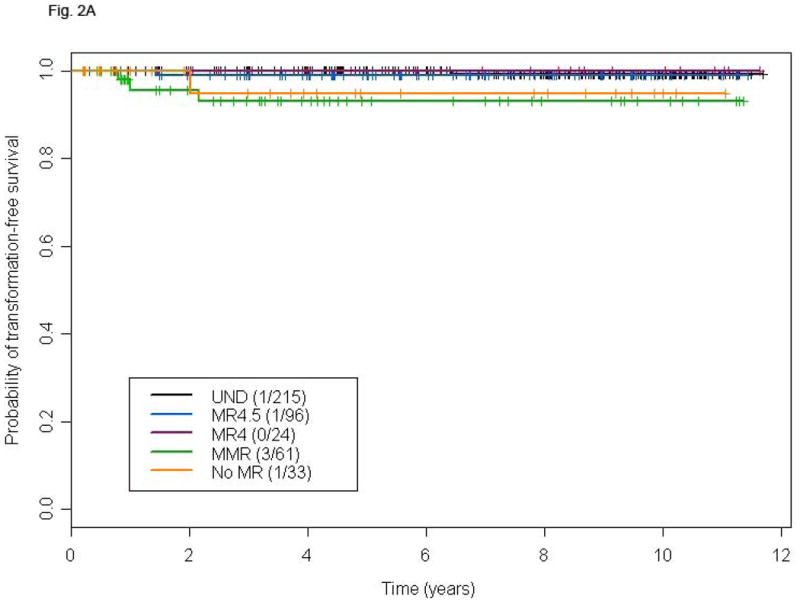
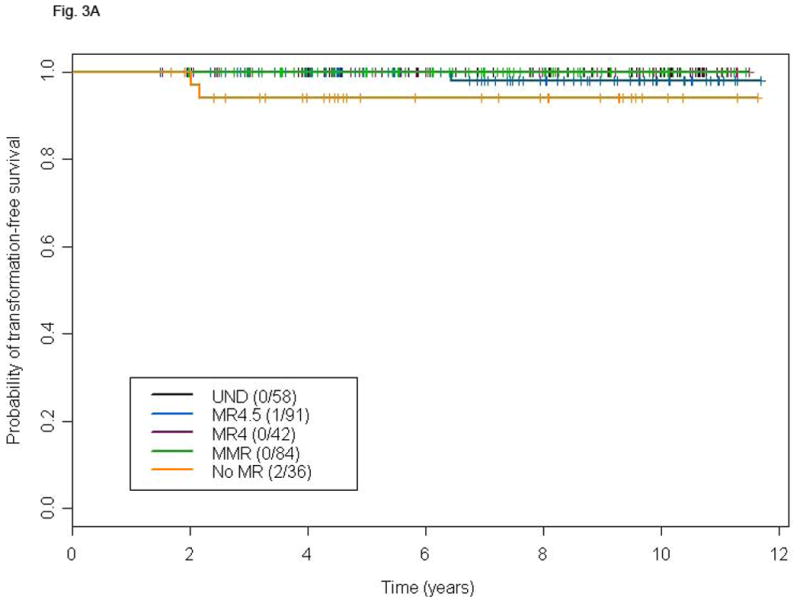
Most patients with chronic myeloid leukemia (CML) in chronic phase (CP) treated with tyrosine kinase inhibitors (TKI) achieve complete cytogenetic response (CCyR). An increasing number of patients also achieve deep molecular responses (MR). We determined the frequency and significance of deep MR after TKI therapy for CML in CP. MR included: major molecular response (MMR), MR4, MR4.5, and undetectable transcripts (UND), i.e., BCR-ABL/ABL of ≤0.1, ≤0.01, ≤0.0032%, and undetectable transcripts, respectively. Four hundred eighty-three patients received imatinib 400 mg/day (IM400, 71, July 2000 to April 2001), imatinib 800 mg/day (IM800, 204, June 2001 to July 2005), nilotinib (106, July 2005 to date), or dasatinib (102, November 2005 to date). UND rates at 36 months were 18.1, 30.6, 29.2, and 28.6%, respectively. Patients achieving UND have superior transformation-free survival (TFS) and overall survival (OS) versus those obtaining ≤MMR, but not other MR levels. At the 18- and 24-month landmark analysis, patients achieving UND have no advantage in TFS and OS compared to those achieving a lesser degree of MR. Among patients achieving MR4.5, those who maintain it for ≥2 years (susMR4·5) have no additional benefit in TFS or OS. Most patients with early CP CML receiving TKI achieve MMR. BCR-ABL transcripts become undetectable in a significant fraction of them. Deeper MR at 18 or 24 months are not associated with a benefit in TFS or OS. Furthermore, achieving susMR4·5 does not appear to further reduce the risk of transformation or death.
大多数接受酪氨酸激酶抑制剂(TKI)治疗的慢性期(CP)慢性髓性白血病(CML)患者可实现完全细胞遗传学反应(CCyR)。越来越多的患者还实现了深度分子反应(MR)。我们确定了 CP 期 CML 接受 TKI 治疗后的深度 MR 的频率和意义。MR 包括:主要分子反应(MMR)、MR4、MR4.5 和不可检测转录本(UND),即 BCR-ABL/ABL 分别为≤0.1、≤0.01、≤0.0032%和不可检测转录本。483 例患者接受伊马替尼 400mg/天(IM400,71 例,2000 年 7 月至 2001 年 4 月)、伊马替尼 800mg/天(IM800,204 例,2001 年 6 月至 2005 年 7 月)、尼洛替尼(106 例,2005 年 7 月至今)或达沙替尼(102 例,2005 年 11 月至今)。36 个月时的 UND 率分别为 18.1%、30.6%、29.2%和 28.6%。与获得≤MMR 的患者相比,达到 UND 的患者具有更好的无转化生存(TFS)和总生存(OS)。在 18 个月和 24 个月的里程碑分析中,与获得较低程度 MR 的患者相比,达到 UND 的患者在 TFS 和 OS 方面没有优势。在达到 MR4.5 的患者中,对于那些持续≥2 年(susMR4·5)保持 MR4.5 的患者,在 TFS 或 OS 方面没有额外获益。大多数接受 TKI 治疗的早期 CP CML 患者可获得 MMR。在其中很大一部分患者中,BCR-ABL 转录本变得不可检测。在 18 或 24 个月时达到更深程度的 MR 与 TFS 或 OS 获益无关。此外,达到 susMR4·5 似乎不会进一步降低转化或死亡的风险。