Department of Thoracic Surgery, Shanghai Pulmonary Hospital, Tongji University; Shanghai First People's Hospital, Shanghai Jiaotong University, Shanghai, China ; Department of Thoracic Surgery, Shanghai Pulmonary Hospital, Tongji University, Shanghai, China.
Ann Thorac Med. 2013 Jul;8(3):170-5. doi: 10.4103/1817-1737.114291.
This study compares early and late outcomes for treatment by video-assisted thoracic surgery (VATS) versus treatment by thoracotomy for clinical N0, but post-operatively unexpected, pathologic N2 disease (cN0-pN2).
Clinical records of patients with unexpected N2 non-small cell lung cancer (NSCLC) who underwent VATS were retrospectively reviewed, and their early and late outcomes were compared to those of patients undergoing conventional thoracotomy during the same period.
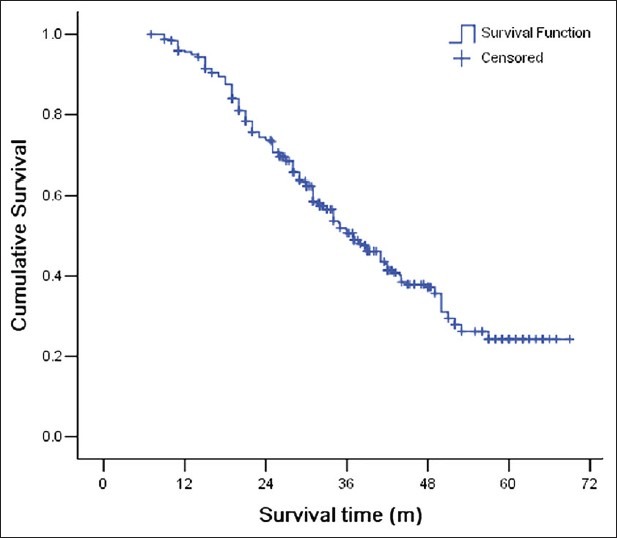
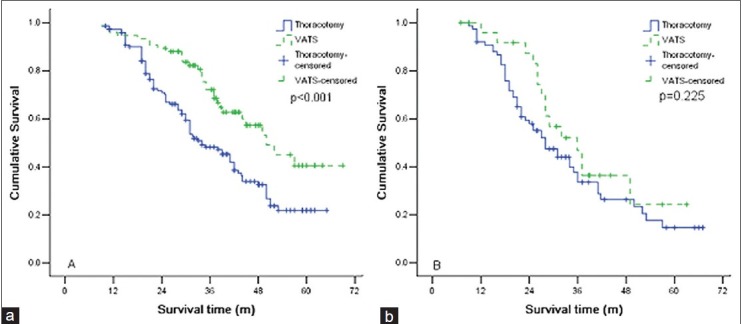
VATS lobectomy took a longer time than thoracotomy (P < 0.001), but removal of thoracic drainage and patient discharge were earlier for patients in the VATS group (P < 0.001). There was no difference in lymph node dissection, mortality and morbidity between the two groups (P > 0.05). The median follow-up time for 287 patients (89.7%) was 37.0 months (range: 7.0-69.0). The VATS group had a longer survival time than for the thoracotomy group (median 49.0 months vs. 31.7 months, P < 0.001). The increased survival time of the VATS group was due to patients with a single station of N2 metastasis (P = 0.001), rather than to patients with multiple stations of N2 metastasis (P = 0.225).
It is both feasible and safe to perform VATS lobectomy on patients with unexpected N2 NSCLC. VATS provides better survival rates for those patients with just one station of metastatic mediastinal lymph nodes.
本研究比较了电视辅助胸腔镜手术(VATS)与开胸手术治疗临床 N0 但术后意外病理 N2 疾病(cN0-pN2)的早期和晚期结果。
回顾性分析了意外 N2 非小细胞肺癌(NSCLC)患者接受 VATS 治疗的临床记录,并将其早期和晚期结果与同期接受常规开胸手术的患者进行比较。
VATS 肺叶切除术耗时比开胸手术长(P<0.001),但 VATS 组患者的胸腔引流管拔除和出院时间更早(P<0.001)。两组间淋巴结清扫、死亡率和发病率无差异(P>0.05)。287 例患者(89.7%)的中位随访时间为 37.0 个月(范围:7.0-69.0)。VATS 组的生存时间长于开胸手术组(中位 49.0 个月比 31.7 个月,P<0.001)。VATS 组生存时间延长的原因是单一纵隔淋巴结转移部位的患者(P=0.001),而不是多个纵隔淋巴结转移部位的患者(P=0.225)。
对意外 N2 NSCLC 患者行 VATS 肺叶切除术是可行且安全的。VATS 为仅有一个转移纵隔淋巴结部位的患者提供了更好的生存率。