Anderson D E, Demissie S, Allaire B T, Bruno A G, Kopperdahl D L, Keaveny T M, Kiel D P, Bouxsein M L
Center for Advanced Orthopaedic Studies, Beth Israel Deaconess Medical Center, 330 Brookline Avenue, RN115, Boston, MA, 02215, USA.
Osteoporos Int. 2014 Feb;25(2):559-66. doi: 10.1007/s00198-013-2452-0. Epub 2013 Aug 8.
We examined how spinal location affects the relationships between quantitative computed tomography (QCT)-based bone measurements and prevalent vertebral fractures. Upper spine (T4-T10) fractures appear to be more strongly related to bone measures than lower spine (T11-L4) fractures, while lower spine measurements are at least as strongly related to fractures as upper spine measurements.
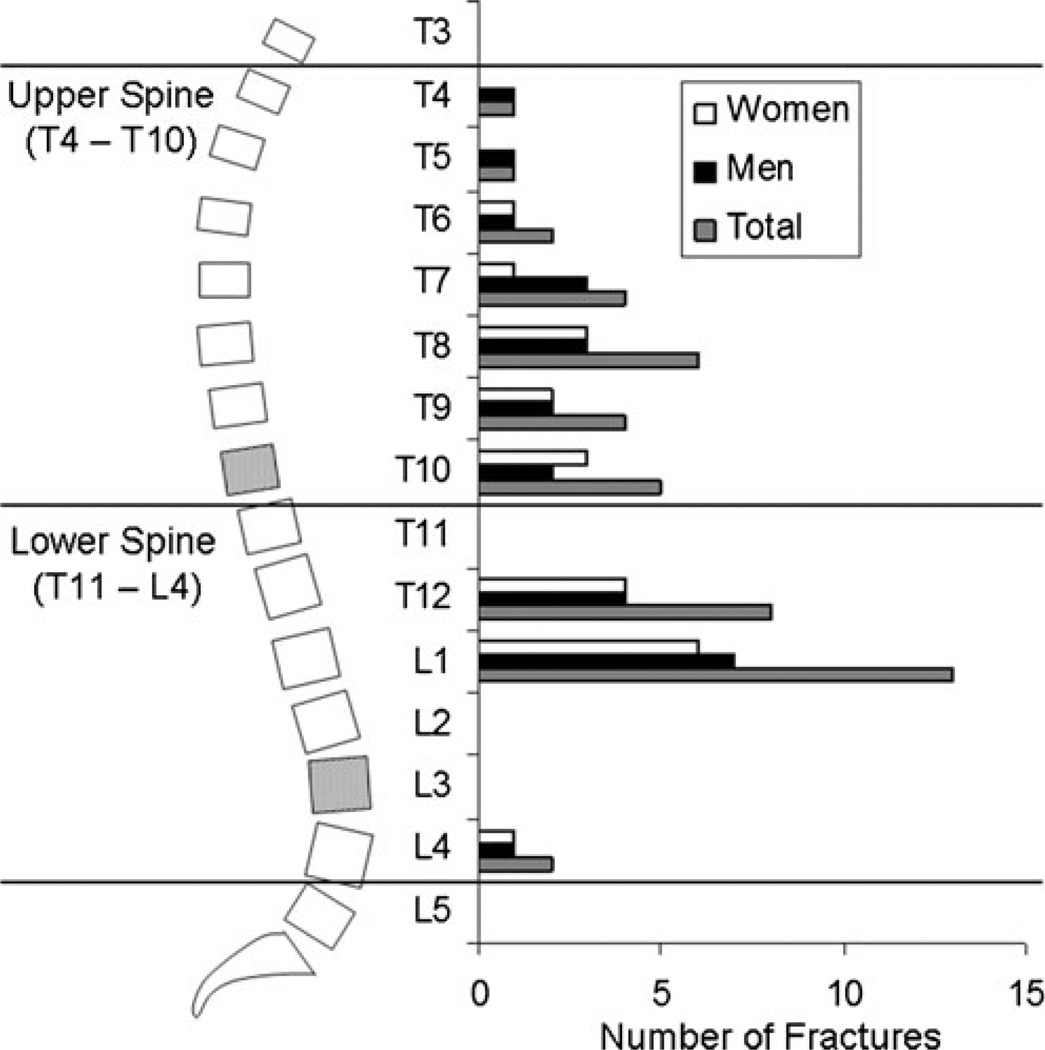
Vertebral fracture (VF), a common injury in older adults, is most prevalent in the mid-thoracic (T7-T8) and thoracolumbar (T12-L1) areas of the spine. However, measurements of bone mineral density (BMD) are typically made in the lumbar spine. It is not clear how the associations between bone measurements and VFs are affected by the spinal locations of both bone measurements and VF.
A community-based case-control study includes 40 cases with moderate or severe prevalent VF and 80 age- and sex-matched controls. Measures of vertebral BMD, strength (estimated by finite element analysis), and factor of risk (load:strength ratio) were determined based on QCT scans at the L3 and T10 vertebrae. Associations were determined between bone measures and prevalent VF occurring at any location, in the upper spine (T4-T10), or in the lower spine (T11-L4).
Prevalent VF at any location was significantly associated with bone measures, with odds ratios (ORs) generally higher for measurements made at L3 (ORs = 1.9-3.9) than at T10 (ORs = 1.5-2.4). Upper spine fracture was associated with these measures at both T10 and L3 (ORs = 1.9-8.2), while lower spine fracture was less strongly associated (ORs = 1.0-2.4) and only reached significance for volumetric BMD measures at L3.
Closer proximity between the locations of bone measures and prevalent VF does not strengthen associations between bone measures and fracture. Furthermore, VF etiology may vary by region, with VFs in the upper spine more strongly related to skeletal fragility.
我们研究了脊柱位置如何影响基于定量计算机断层扫描(QCT)的骨测量与现患椎体骨折之间的关系。上脊柱(T4 - T10)骨折似乎比下脊柱(T11 - L4)骨折与骨测量的关系更密切,而下脊柱测量与骨折的关系至少与上脊柱测量一样密切。
椎体骨折(VF)是老年人常见的损伤,在脊柱的中胸段(T7 - T8)和胸腰段(T12 - L1)最为普遍。然而,骨密度(BMD)测量通常在腰椎进行。目前尚不清楚骨测量与椎体骨折之间的关联如何受到骨测量和椎体骨折的脊柱位置的影响。
一项基于社区的病例对照研究包括40例患有中度或重度现患椎体骨折的病例和80例年龄及性别匹配的对照。基于L3和T10椎体的QCT扫描确定椎体骨密度、强度(通过有限元分析估计)和风险因素(负荷:强度比)的测量值。确定骨测量与任何位置、上脊柱(T4 - T10)或下脊柱(T11 - L4)发生的现患椎体骨折之间的关联。
任何位置的现患椎体骨折与骨测量显著相关,L3处测量的比值比(OR)通常高于T10处(OR = 1.9 - 3.9对比OR = 1.5 - 2.4)。上脊柱骨折在T10和L3处均与这些测量相关(OR = 1.9 - 8.2),而下脊柱骨折的相关性较弱(OR = 1.0 - 2.4),仅在L3处的体积骨密度测量中达到显著水平。
骨测量位置与现患椎体骨折位置之间的距离更近并不会加强骨测量与骨折之间的关联。此外,椎体骨折的病因可能因区域而异,上脊柱的椎体骨折与骨骼脆性的关系更强。