Kennedy Sidney H
University Health Network, University of Toronto, Ontario, Canada.
Prim Care Companion CNS Disord. 2013;15(2). doi: 10.4088/PCC.12r01420. Epub 2013 Apr 11.
To provide general practitioners with a comparison of major depressive disorder treatments received in primary care and psychiatric clinic settings, a focus on treatment outcomes related to currently prescribed antidepressants, and a review of new and emerging therapeutic strategies.
English-language evidence-based guidelines and peer-reviewed literature published between January 1, 2005, and December 31, 2011, were identified using PubMed, MEDLINE, and EMBASE. All searches contained the terms major depressive disorder and unipolar depression, and excluded the terms bipolar disorder/manic depressive disorder. The following search terms were also included: naturalistic study, antidepressant, relapse, recurrence, residual symptoms, response, remission, sequential medication trials, and treatment-resistant depression.
Meta-analyses, systematic reviews, and practice guidelines were included. Bibliographies were used to identify additional articles of interest.
Abstracts and articles were screened for relevance to primary care practice. Population-based studies and those involving patients treated in primary care were used whenever possible.
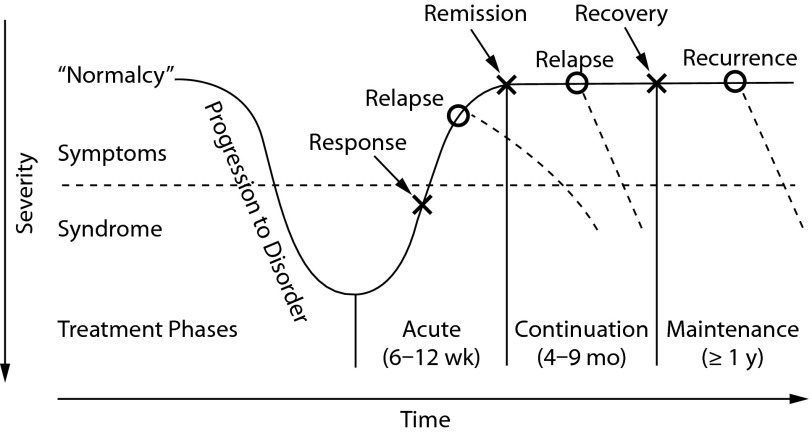
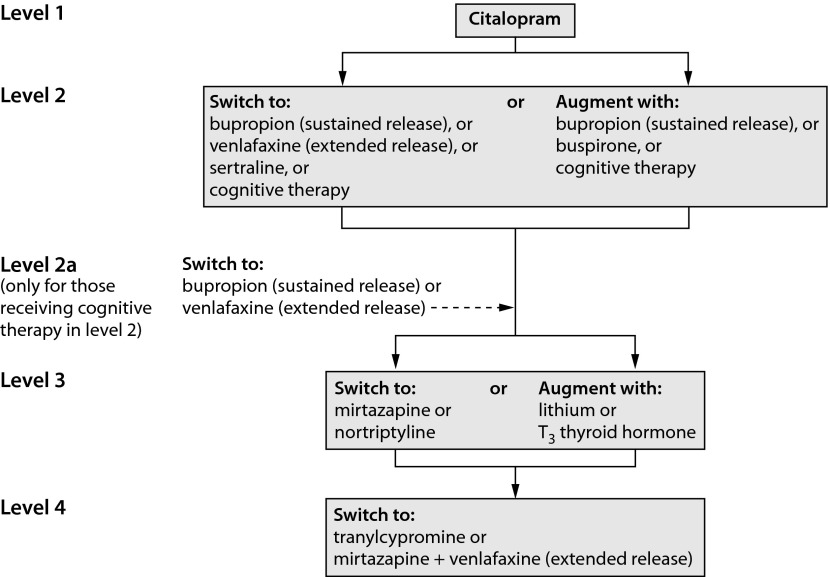
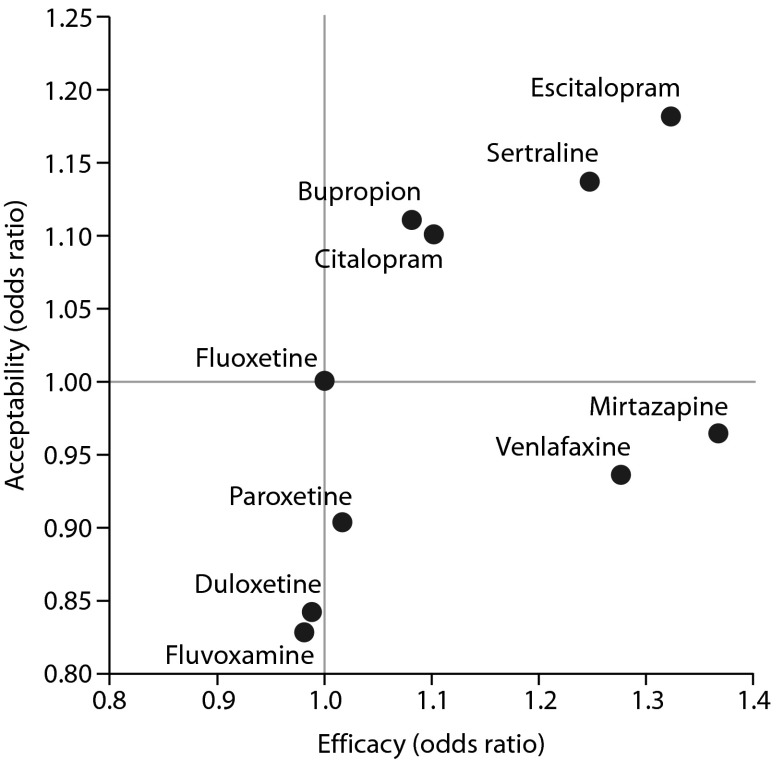
Achieving remission from a major depressive episode is important to improve functional outcomes and to reduce relapse and recurrence. Despite the availability of numerous antidepressants, as many as 50% of patients require treatment modifications beyond first-line therapy. Among remitters, 90% report residual symptoms that may interfere with function. Patients treated in primary care often have chronic depression (symptom duration ≥ 24 months at presentation) and medical comorbidities. These are clinical predictors of worse outcomes and require individualized attention when treatment is initiated. Antidepressants differ in efficacy, tolerability, and side effects-factors that may affect adherence to treatment.
Major depressive disorder is highly prevalent in primary care and is among the most common causes of loss of disability-adjusted life-years worldwide. There are few differences in clinical profiles between depressed patients in primary care and those in specialist clinics, although differences in symptoms and comorbid conditions among individual depressed patients present a challenge for the physician providing individualized treatment. The goal of treatment is remission with good functional and psychosocial outcomes. Physicians in primary care should have expertise in working with a number of current antidepressant approaches and an awareness of new and emerging treatments.
为全科医生提供在初级保健和精神科诊所接受的重度抑郁症治疗的比较,重点关注与当前处方抗抑郁药相关的治疗结果,并综述新出现的治疗策略。
使用PubMed、MEDLINE和EMBASE检索2005年1月1日至2011年12月31日期间发表的英文循证指南和同行评审文献。所有检索词均包含重度抑郁症和单相抑郁症,排除双相情感障碍/躁狂抑郁症相关词汇。还纳入了以下检索词:自然主义研究、抗抑郁药、复发、再发、残留症状、反应、缓解、序贯药物试验和难治性抑郁症。
纳入荟萃分析、系统评价和实践指南。通过参考文献目录确定其他相关文章。
筛选摘要和文章,以确定与初级保健实践的相关性。尽可能使用基于人群的研究以及涉及在初级保健中接受治疗的患者的研究。
从重度抑郁发作中实现缓解对于改善功能结局以及减少复发和再发很重要。尽管有多种抗抑郁药可供使用,但多达50%的患者需要一线治疗以外的治疗调整。在缓解者中,90%报告有可能干扰功能的残留症状。在初级保健中接受治疗的患者通常患有慢性抑郁症(就诊时症状持续时间≥24个月)和合并症。这些是预后较差的临床预测因素,在开始治疗时需要个体化关注。抗抑郁药在疗效、耐受性和副作用方面存在差异,这些因素可能会影响治疗依从性。
重度抑郁症在初级保健中非常普遍,是全球残疾调整生命年损失的最常见原因之一。初级保健中的抑郁症患者与专科诊所中的患者在临床特征上几乎没有差异,尽管个体抑郁症患者的症状和合并症差异给提供个体化治疗的医生带来了挑战。治疗的目标是实现缓解并获得良好的功能和心理社会结局。初级保健医生应具备使用多种当前抗抑郁治疗方法的专业知识,并了解新出现的治疗方法。