Ahmad Dina S, Esmadi Mohammad, Steinmann William C
Department of Internal Medicine, University of Missouri School of Medicine, Columbia, MO, USA.
Avicenna J Med. 2013 Apr;3(2):37-47. doi: 10.4103/2231-0770.114121.
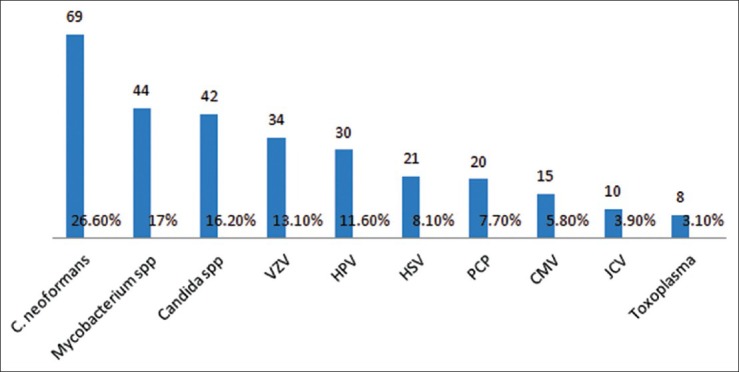
Idiopathic CD4 lymphocytopenia (ICL) was first defined in 1992 by the US Centers for Disease Control and Prevention (CDC) as the repeated presence of a CD4+ T lymphocyte count of fewer than 300 cells per cubic millimeter or of less than 20% of total T cells with no evidence of human immunodeficiency virus (HIV) infection and no condition that might cause depressed CD4 counts. Most of our knowledge about ICL comes from scattered case reports. The aim of this study was to collect comprehensive data from the previously published cases to understand the characteristics of this rare condition. We searched the PubMed database and Science Direct for case reports since 1989 for Idiopathic CD4 lymphocytopenia cases. We found 258 cases diagnosed with ICL in 143 published papers. We collected data about age, sex, pathogens, site of infections, CD4 count, CD8 count, CD4:CD8 ratio, presence of HIV risk factors, malignancies, autoimmune diseases and whether the patients survived or died. The mean age at diagnosis of first opportunistic infection (or ICL if no opportunistic infection reported) was 40.7 ± 19.2 years (standard deviation), with a range of 1 to 85. One-sixty (62%) patients were males, 91 (35.2%) were females, and 7 (2.7%) patients were not identified whether males or females. Risk factors for HIV were documented in 36 (13.9%) patients. The mean initial CD4 count was 142.6 ± 103.9/mm(3) (standard deviation). The mean initial CD8 count was 295 ± 273.6/mm(3) (standard deviation). The mean initial CD4:CD8 ratio was 0.6 ± 0.7 (standard deviation). The mean lowest CD4 count was 115.4 ± 87.1/mm(3) (standard deviation). The majority of patients 226 (87.6%) had at least one infection. Cryptococcal infections were the most prevalent infections in ICL patients (26.6%), followed by mycobacterial infections (17%), candidal infections (16.2%), and VZV infections (13.1%). Malignancies were reported in 47 (18.1%) patients. Autoimmune diseases were reported in 37 (14.2%) patients.
特发性CD4淋巴细胞减少症(ICL)于1992年首次由美国疾病控制与预防中心(CDC)定义为:CD4 + T淋巴细胞计数反复低于每立方毫米300个细胞,或低于总T细胞的20%,且无人类免疫缺陷病毒(HIV)感染证据,也无可能导致CD4计数降低的疾病。我们对ICL的了解大多来自零散的病例报告。本研究的目的是从先前发表的病例中收集全面数据,以了解这种罕见疾病的特征。我们在PubMed数据库和Science Direct中搜索了自1989年以来关于特发性CD4淋巴细胞减少症病例的报告。我们在143篇已发表论文中发现了258例诊断为ICL的病例。我们收集了有关年龄、性别、病原体、感染部位、CD4计数、CD8计数、CD4:CD8比值、HIV危险因素的存在情况、恶性肿瘤、自身免疫性疾病以及患者存活或死亡情况的数据。首次机会性感染(或若未报告机会性感染则为ICL)诊断时的平均年龄为40.7±19.2岁(标准差),范围为1至85岁。160例(62%)患者为男性,91例(35.2%)为女性,7例(2.7%)患者未明确性别。36例(13.9%)患者记录有HIV危险因素。初始CD4平均计数为142.6±103.9/mm³(标准差)。初始CD8平均计数为295±273.6/mm³(标准差)。初始CD4:CD8平均比值为0.6±0.7(标准差)。最低CD4平均计数为115.4±87.1/mm³(标准差)。大多数患者226例(87.6%)至少有一次感染。隐球菌感染是ICL患者中最常见(26.6%)的感染,其次是分枝杆菌感染(17%)、念珠菌感染(16.2%)和水痘带状疱疹病毒感染(13.1%)。47例(18.1%)患者报告有恶性肿瘤。3例(14.2%)患者报告有自身免疫性疾病。