Chhabra Gaurav, Sharma Subhadra, Subramanian Arulselvi, Agrawal Deepak, Sinha Sumit, Mukhopadhyay Asok K
Department of Laboratory Medicine, Jai Prakash Narayan Apex Trauma Centre, All India Institute of Medical Sciences, New Delhi, India.
J Emerg Trauma Shock. 2013 Jul;6(3):180-5. doi: 10.4103/0974-2700.115332.
Coagulopathy frequently occurs following traumatic brain injury (TBI) and usually occurs 6-72 hour post-trauma. The incidence and the probable risk factors for development of coagulopathy and poor outcome following TBI are largely unknown and vary considerably.
To assess the incidence and probable risk factors for development of coagulopathy and to identify the risk factors for poor outcome in terms of median survival time following TBI.
In this prospective study over two years, patients of isolated moderate and severe traumatic brain injury (GCS≤12) admitted to trauma center had coagulation profile (PT, APTT, thrombin time, fibrinogen and D-dimer), arterial lactate and ABG analysis done on day of admission and on day three. Coagulopathy was defined as prothrombin time (PT) or/and activated partial thromboplastin time (APTT) more than 1.5 times the normal control. Incidence of in-hospital mortality was assessed in all cases.
A stepwise logistic regression analysis was performed to identify risk factors for coagulopathy and mortality in these patients.
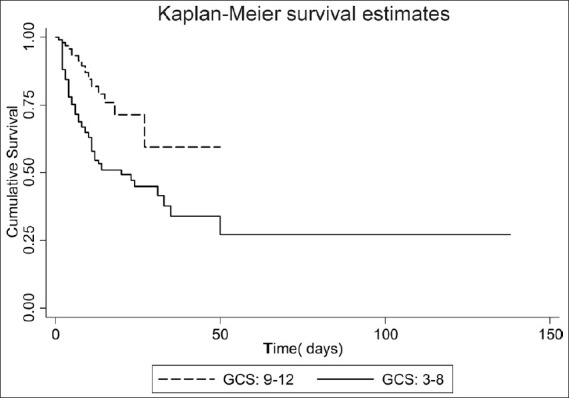
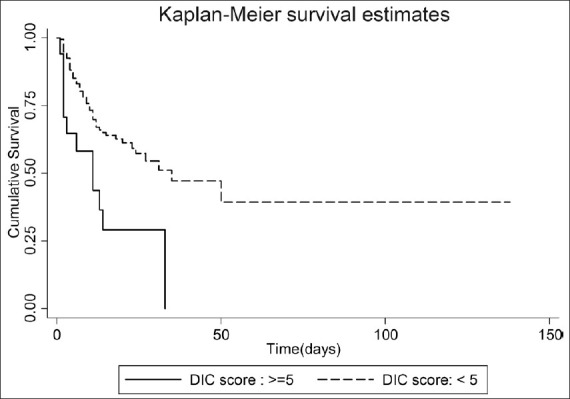
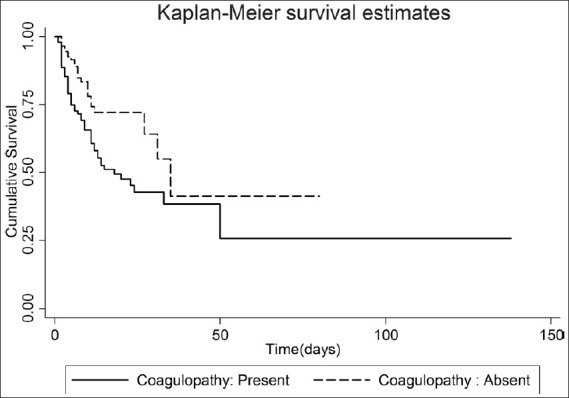
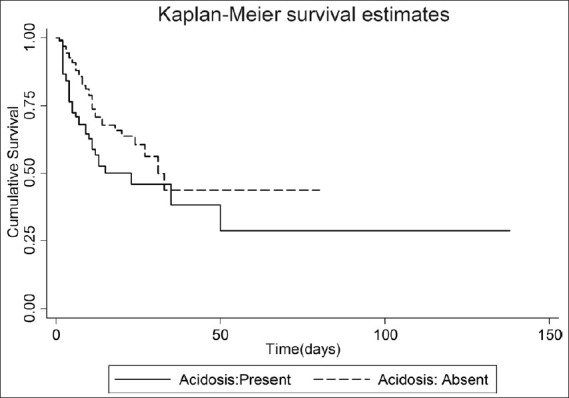
A total of 208 patients were enrolled in the study. The mean age was 32 ± 12 years and mean GCS was 7.1 ± 2.8. Coagulopathy was present in 46% (n = 96) of patients. Risk factors for development of coagulopathy were found out to be severity of head injury (OR: 2.81), elevated D-dimer (OR: 3.43), low hemoglobin (OR: 3.13), and effaced cisterns in the CT scan (OR: 2.72). Presence of coagulopathy (OR: 2.97) and severity of head injury (OR: 5.70) strongly predicted poor outcome, and were associated with a decreased median survival time.
There is a high incidence of coagulopathy following TBI. The presence of coagulopathy as well as of severity of TBI are strong predictors of in-hospital mortality in these patients.
凝血功能障碍常在创伤性脑损伤(TBI)后出现,通常发生在创伤后6 - 72小时。TBI后凝血功能障碍的发生率以及其发生和不良预后的可能危险因素在很大程度上尚不清楚,且差异很大。
评估凝血功能障碍的发生率和可能的危险因素,并根据TBI后的中位生存时间确定不良预后的危险因素。
在这项为期两年的前瞻性研究中,入住创伤中心的单纯中度和重度创伤性脑损伤(格拉斯哥昏迷量表评分≤12分)患者在入院当天和第三天进行凝血指标(凝血酶原时间、活化部分凝血活酶时间、凝血酶时间、纤维蛋白原和D - 二聚体)、动脉血乳酸和动脉血气分析。凝血功能障碍定义为凝血酶原时间(PT)或/和活化部分凝血活酶时间(APTT)超过正常对照的1.5倍。评估所有病例的院内死亡率。
进行逐步逻辑回归分析以确定这些患者凝血功能障碍和死亡率的危险因素。
共有208例患者纳入研究。平均年龄为32±12岁,平均格拉斯哥昏迷量表评分为7.1±2.8。46%(n = 96)的患者存在凝血功能障碍。发现凝血功能障碍的危险因素为头部损伤严重程度(比值比:2.81)、D - 二聚体升高(比值比:3.43)、血红蛋白降低(比值比:3.13)以及CT扫描显示脑池消失(比值比:2.72)。凝血功能障碍(比值比:2.97)和头部损伤严重程度(比值比:5.70)强烈预测不良预后,并与中位生存时间缩短相关。
TBI后凝血功能障碍的发生率很高。凝血功能障碍的存在以及TBI的严重程度是这些患者院内死亡率的强有力预测指标。