Yeung Jacky T, Williams Jessica, Bowling William M
Department of Surgery, Michigan State University College of Human Medicine, East Lansing, USA.
J Emerg Trauma Shock. 2013 Jul;6(3):189-94. doi: 10.4103/0974-2700.115337.
Animal and molecular studies have shown that cocaine exerts a neuroprotective effect against cerebral ischemia.
To determine if the presence of cocaine metabolites on admission following traumatic brain injury (TBI) is associated with better outcomes.
Level-1 trauma center, retrospective cohort.
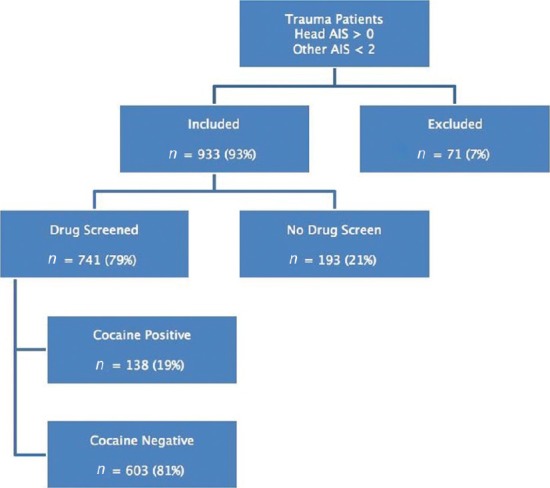
After obtaining Institutional Review Board (IRB) approval, the trauma registry was searched from 2006 to 2009 for all patients aged 15-55 years with blunt head trauma and non-head AIS <3. Exclusion criteria were pre-existing brain pathology and death within 30 min of admission. The primary outcome was in-hospital mortality; secondary outcomes were hospital length of stay (LOS), and Glasgow Outcome Score (GOS).
Logistic regression was used to determine the independent effect of cocaine on mortality. Hospital LOS was compared with multiple linear regression.
A total of 741 patients met criteria and had drug screens. The screened versus unscreened groups were similar. Cocaine positive patients were predominantly African-American (46% vs. 21%, P < 0.0001), older (40 years vs. 30 years, P < 0.0001), and had ethanol present more often (50.7% vs. 37.8%, P = 0.01). There were no differences in mortality (cocaine-positive 1.4% vs. cocaine-negative 2.7%, P = 0.6) on both univariate and multivariate analysis.
Positive cocaine screening was not associated with mortality in TBI. An effect may not have been detected because of the low mortality rate. LOS is affected by many factors unrelated to the injury and may not be a good surrogate for recovery. Similarly, GOS may be too coarse a measure to identify a benefit.
动物和分子研究表明,可卡因对脑缺血具有神经保护作用。
确定创伤性脑损伤(TBI)入院时可卡因代谢物的存在是否与更好的预后相关。
一级创伤中心,回顾性队列研究。
获得机构审查委员会(IRB)批准后,检索2006年至2009年创伤登记处中所有年龄在15 - 55岁、头部钝器伤且非头部简明损伤定级标准(AIS)<3的患者。排除标准为既往存在脑部病变以及入院后30分钟内死亡。主要结局是院内死亡率;次要结局是住院时间(LOS)和格拉斯哥预后评分(GOS)。
采用逻辑回归确定可卡因对死亡率的独立影响。通过多元线性回归比较住院时间。
共有741名患者符合标准并进行了药物筛查。筛查组与未筛查组相似。可卡因阳性患者主要为非裔美国人(46%对21%,P < 0.0001),年龄较大(40岁对30岁,P < 0.0001),且乙醇检测呈阳性的情况更常见(50.7%对37.8%,P = 0.01)。单因素和多因素分析中,死亡率均无差异(可卡因阳性1.4%对可卡因阴性2.7%,P = 0.6)。
TBI患者中可卡因筛查呈阳性与死亡率无关。可能由于死亡率低而未检测到其影响。住院时间受许多与损伤无关的因素影响,可能不是恢复情况的良好替代指标。同样,GOS可能过于粗略,无法确定是否存在益处。