Bartlett Eric S, Walters Thomas D, Yu Eugene
Princess Margaret Cancer Centre, Joint Department of Medical Imaging, University of Toronto, 610 University Avenue, Room 3-956, Toronto, ON, Canada M5G 2M9.
ISRN Otolaryngol. 2013 Jul 24;2013:232968. doi: 10.1155/2013/232968. eCollection 2013.
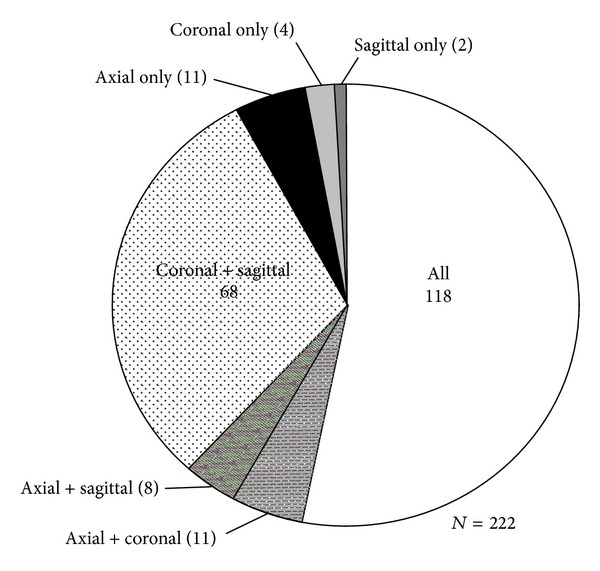
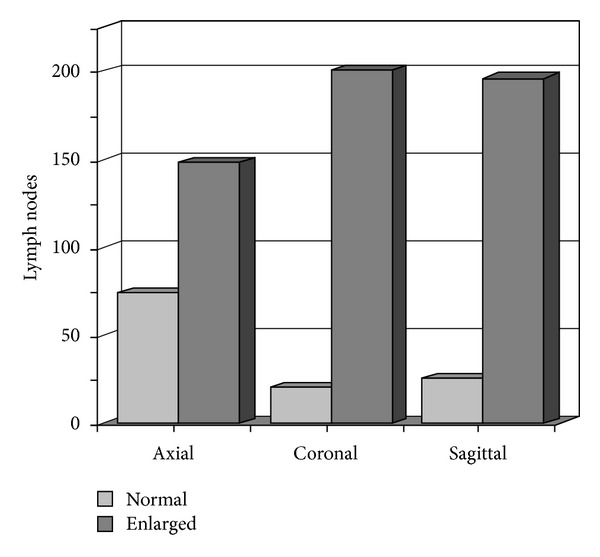
Objective. We evaluate if axial-based lymph node size criteria can be applied to coronal and sagittal planes. Methods. Fifty pretreatment computed tomographic (CT) neck exams were evaluated in patients with head and neck squamous cell carcinoma (SCCa) and neck lymphadenopathy. Axial-based size criteria were applied to all 3 imaging planes, measured, and classified as "enlarged" if equal to or exceeding size criteria. Results. 222 lymph nodes were "enlarged" in one imaging plane; however, 53.2% (118/222) of these were "enlarged" in all 3 planes. Classification concordance between axial versus coronal/sagittal planes was poor (kappa = -0.09 and -0.07, resp., P < 0.05). The McNemar test showed systematic misclassification when comparing axial versus coronal (P < 0.001) and axial versus sagittal (P < 0.001) planes. Conclusion. Classification of "enlarged" lymph nodes differs between axial versus coronal/sagittal imaging planes when axial-based nodal size criteria are applied independently to all three imaging planes, and exclusively used without other morphologic nodal data.
目的。我们评估基于轴位的淋巴结大小标准是否可应用于冠状面和矢状面。方法。对50例头颈部鳞状细胞癌(SCCa)合并颈部淋巴结病患者的术前颈部计算机断层扫描(CT)检查进行评估。将基于轴位的大小标准应用于所有三个成像平面,进行测量,若等于或超过大小标准则分类为“增大”。结果。222个淋巴结在一个成像平面上“增大”;然而,其中53.2%(118/222)在所有三个平面上均“增大”。轴位与冠状面/矢状面之间的分类一致性较差(kappa分别为 -0.09和 -0.07,P < 0.05)。McNemar检验显示,在比较轴位与冠状面(P < 0.001)以及轴位与矢状面(P < 0.001)平面时存在系统性错误分类。结论。当将基于轴位的淋巴结大小标准独立应用于所有三个成像平面且仅在不使用其他淋巴结形态学数据的情况下使用时,轴位与冠状面/矢状面成像平面之间“增大”淋巴结的分类存在差异。