University of California and Veterans' Affairs Medical Centers, San Diego, California, USA.
Can J Cardiol. 2013 Oct;29(10):1218-26. doi: 10.1016/j.cjca.2013.07.672. Epub 2013 Aug 30.
Pulmonary vein (PV) isolation has disappointing results in patients with obesity, heart failure, obstructive sleep apnea (OSA) and enlarged left atria (LA), for unclear reasons. We hypothesized that these comorbidities may cause higher numbers or non-PV locations of atrial fibrillation (AF) sources, where targeted source ablation (focal impulse and rotor modulation [FIRM]) should improve the single-procedure success of ablation.
The Conventional Ablation of AF With or Without Focal Impulse and Rotor Modulation (CONFIRM) trial prospectively enrolled 92 patients at 107 AF ablation procedures, in whom computational mapping identified AF rotors or focal sources. Patients underwent FIRM plus conventional ablation (FIRM-guided), or conventional ablation only, and were evaluated for recurrent AF quarterly with rigourous, often implanted, monitoring. We report the n = 73 patients undergoing first ablation in whom demographic information was available (n = 52 conventional, n = 21 FIRM-guided).
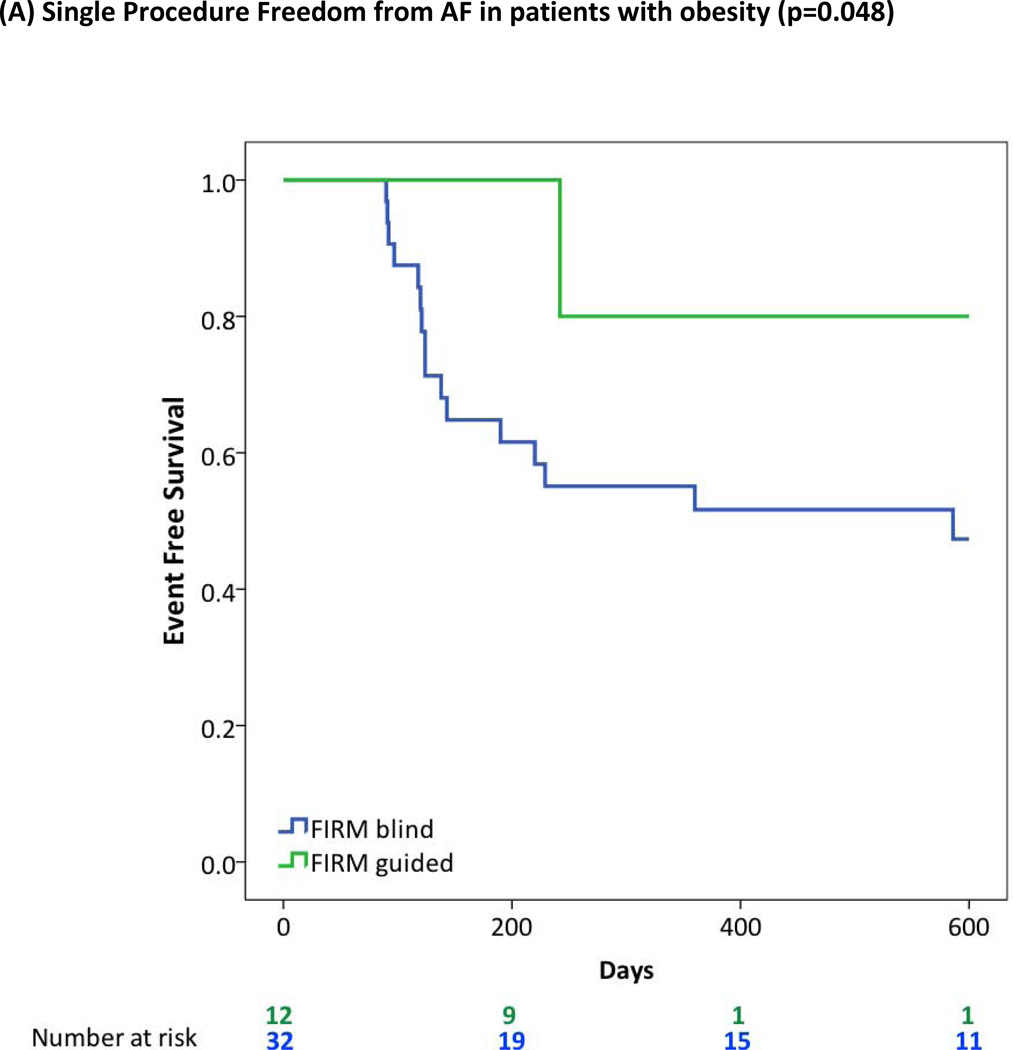
Stable sources for AF were found in 97.1% of patients. The numbers of concurrent sources per patient (2.1 ± 1.1) rose with LA diameter (P = 0.021), lower left ventricular ejection fraction (P = 0.039), and the presence of OSA (P = 0.002) or hypomagnesemia (P = 0.017). Right atrial sources were associated with obesity (body mass index ≥ 30; P = 0.015). In patients with obesity, hypertension, OSA, and LA diameter > 40 mm, single-procedure freedom from AF was > 80% when FIRM-guided was used vs. < 50% when conventional ablation was used (all; P < 0.05).
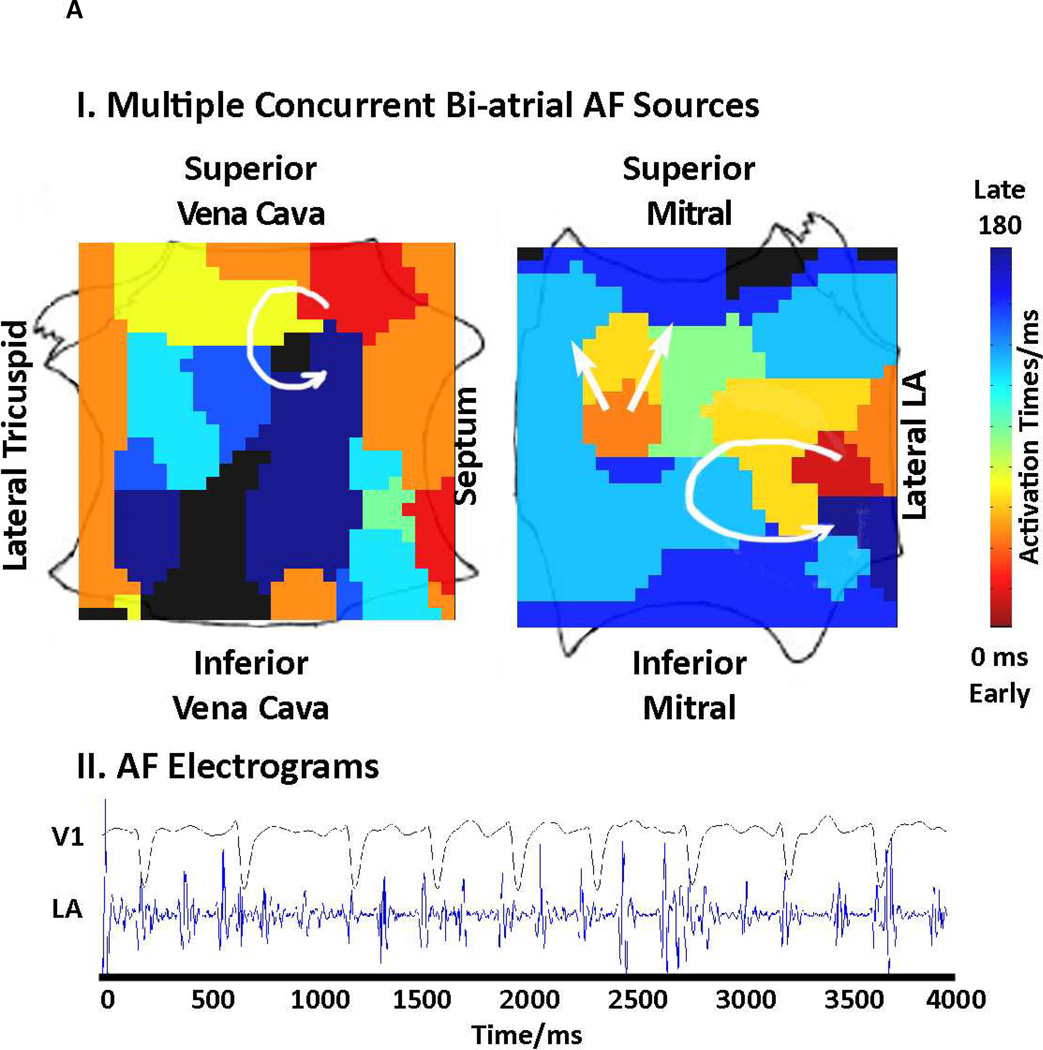
Patients with "difficult to treat" AF exhibit more concurrent AF sources in more widespread biatrial distributions than other patients. These mechanisms explain the disappointing results of PV isolation, and how FIRM can identify patient-specific AF sources to enable successful ablation in this population.
肺静脉(PV)隔离在肥胖、心力衰竭、阻塞性睡眠呼吸暂停(OSA)和左心房(LA)增大的患者中效果不佳,原因尚不清楚。我们假设这些合并症可能导致更多的房颤(AF)源或非 PV 位置,在这些位置进行靶向源消融(局灶冲动和转子调制[FIRM])应该提高消融的单次手术成功率。
常规消融房颤伴或不伴局灶冲动和转子调制(CONFIRM)试验前瞻性纳入了 92 名患者的 107 次房颤消融手术,其中计算映射识别房颤转子或局灶源。患者接受 FIRM 加常规消融(FIRM 引导)或仅常规消融,并通过严格、常植入的监测每季度评估复发性 AF。我们报告了 n = 73 名接受首次消融的患者的信息(n = 52 例常规消融,n = 21 例 FIRM 引导)。
97.1%的患者发现稳定的房颤源。每位患者并发源的数量(2.1 ± 1.1)随左心房直径增加(P = 0.021)、左心室射血分数降低(P = 0.039)、OSA 存在(P = 0.002)或低镁血症(P = 0.017)而增加。右房源与肥胖(体重指数≥30;P = 0.015)有关。在肥胖、高血压、OSA 和 LA 直径>40mm 的患者中,当使用 FIRM 引导时,单次手术 AF 无复发率>80%,而当使用常规消融时<50%(均为 P<0.05)。
“难以治疗”的 AF 患者比其他患者表现出更多的并发 AF 源,且分布更广泛。这些机制解释了 PV 隔离效果不佳的原因,以及 FIRM 如何识别特定于患者的 AF 源,从而使该人群的消融成功。