Department of Family Medicine and Emergency Medicine, Université Laval, Centre de Recherché du Le Centre Hospitalier Universitaire de Québec, 9 rue McMahon, Local 1899-6, Quebec, Quebec City, Quebec QC G1R 2J6, Canada.
Br J Cancer. 2013 Oct 15;109(8):2066-71. doi: 10.1038/bjc.2013.515. Epub 2013 Sep 24.
For evidence-based medical practice, well-defined risk scoring systems are essential to identify patients with a poor prognosis. The objective of this study was to develop a prognostic score, the Montreal prognostic score (MPS), to improve prognostication of patients with incurable non-small cell lung cancer (NSCLC) in everyday practice.
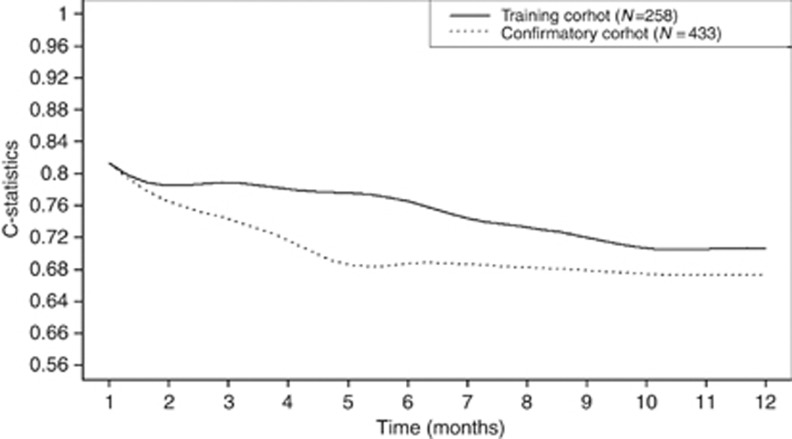
A training cohort (TC) and a confirmatory cohort (CC) of newly diagnosed patients with NSCLC planning to receive chemotherapy were used to develop the MPS. Stage and clinically available biomarkers were entered into a Cox model and risk weights were estimated. C-statistics were used to test the accuracy.
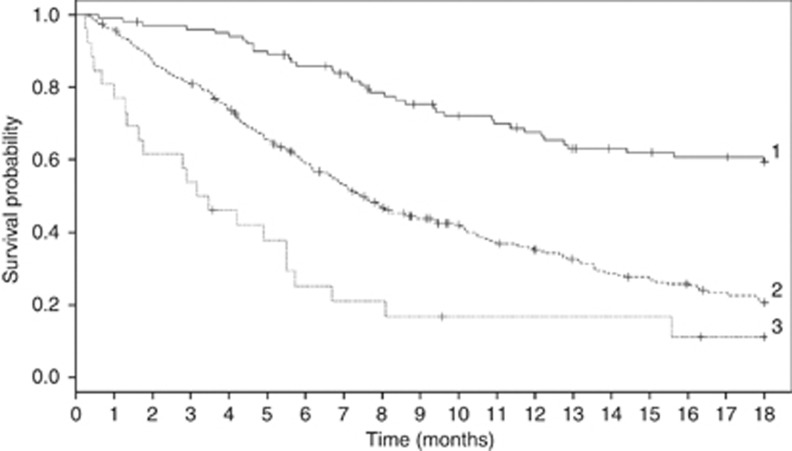
The TC consisted of 258 patients and the CC consisted of 433 patients. Montreal prognostic score classified patients into three distinct groups with median survivals of 2.5 months (95% confidence interval (CI): 1.8, 4.2), 8.2 months (95% CI: 7.0, 9.4) and 18.2 months (95% CI: 14.0, 27.5), respectively (log-rank, P<0.001). Overall, the C-statistics were 0.691 (95% CI: 0.685, 0.697) for the TC and 0.665 (95% CI: 0.661, 0.670) for the CC.
The MPS, by classifying patients into three well-defined prognostic groups, provides valuable information, which physicians could use to better inform their patients about treatment options, especially the best timing to involve palliative care teams.
为了进行循证医学实践,明确界定的风险评分系统对于识别预后不良的患者至关重要。本研究的目的是开发一种预后评分系统,即蒙特利尔预后评分(MPS),以改善无法治愈的非小细胞肺癌(NSCLC)患者的预后预测。
使用新诊断为计划接受化疗的 NSCLC 患者的训练队列(TC)和验证队列(CC)来开发 MPS。将分期和临床可用的生物标志物纳入 Cox 模型,并估计风险权重。C 统计量用于测试准确性。
TC 由 258 例患者组成,CC 由 433 例患者组成。MPS 将患者分为三个不同的组,中位生存期分别为 2.5 个月(95%置信区间:1.8,4.2)、8.2 个月(95%置信区间:7.0,9.4)和 18.2 个月(95%置信区间:14.0,27.5)(对数秩检验,P<0.001)。总体而言,TC 的 C 统计量为 0.691(95%置信区间:0.685,0.697),CC 的 C 统计量为 0.665(95%置信区间:0.661,0.670)。
MPS 通过将患者分为三个明确的预后组,提供了有价值的信息,医生可以利用这些信息更好地向患者提供治疗选择的信息,特别是何时最好让姑息治疗团队介入。