Authors' Affiliation: Fox Chase Cancer Center, Philadelphia, Pennsylvania.
Clin Cancer Res. 2013 Dec 1;19(23):6633-43. doi: 10.1158/1078-0432.CCR-13-0152. Epub 2013 Oct 2.
Multimodality treatment of squamous cell carcinoma of the head and neck (SCCHN) often involves radiotherapy and cisplatin-based therapy. Elevated activity of DNA repair mechanisms, such as the nucleotide excision repair (NER) pathway, of which ERCC1 is a rate-limiting element, are associated with cisplatin and possibly RT resistance. We have determined excision repair cross-complementing group 1 (ERCC1) expression in human papillomavirus (HPV)-negative SCCHN treated with surgery [± adjuvant radiotherapy/chemoradiation (CRT)].
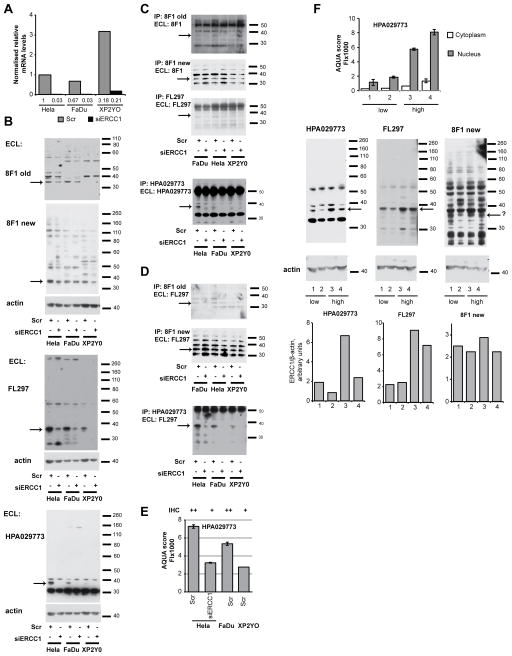
We assessed ERCC1 protein expression in archival tumors using immunofluorescence staining and automatic quantitative analysis (AQUA) with three antibodies to ERCC1 (8F1, FL297, and HPA029773). Analysis with Classification and Regression Tree (CART) methods ascertained the cutoff points between high/low ERCC1 expression. Multivariable analysis adjusted for age, T, and N stage. Kaplan-Meier curves determined median survival. ERCC1 expression at initial tumor presentation and in recurrent disease were compared. Performance characteristics of antibodies were assessed.
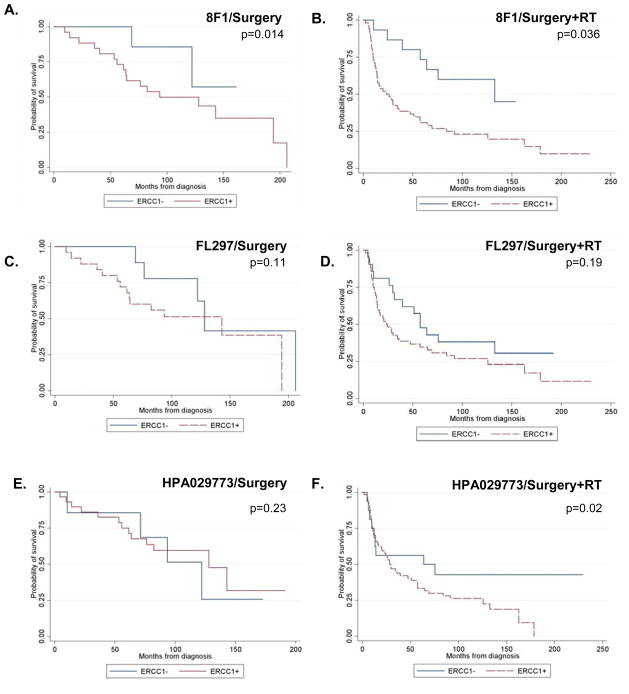
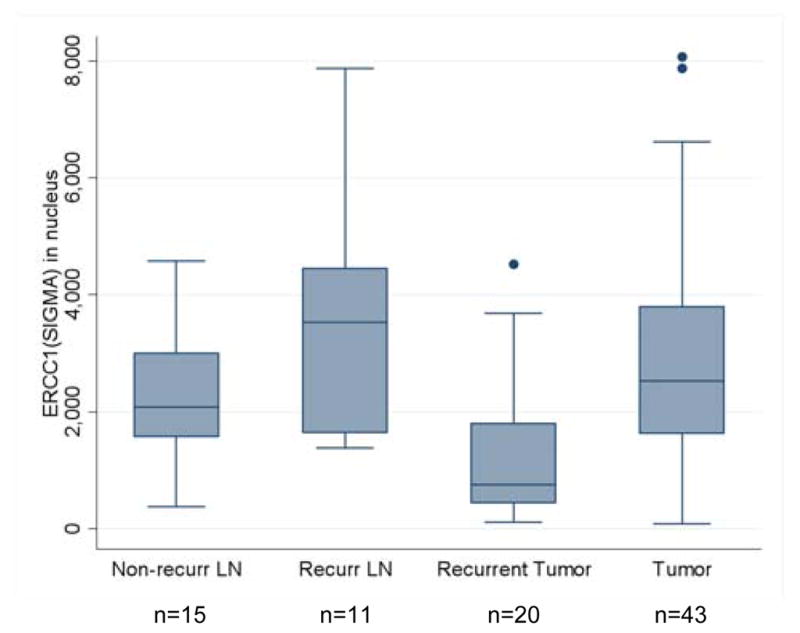
ERCC1 low/high groups were defined on the basis of AQUA analysis with 8F1/2009, FL297, and HPA029773. Among patients treated with surgery plus adjuvant radiotherapy/CRT, longer median survival was observed in ERCC1-low versus ERCC1-high tumors (64 vs. 29 months; P = 0.02; HPA029773). Data obtained with HPA029773 indicated no survival difference among patients treated only with surgery. Recurrent cancers had lower ERCC1 AQUA scores than tumors from initial presentation. Extensive characterization indicated optimal specificity and performance by the HPA029773 antibody.
Using AQUA, with the specific ERCC1 antibody HPA029773, we found a statistical difference in survival among high/low-ERCC1 tumors from patients treated with surgery and adjuvant radiotherapy.
头颈部鳞状细胞癌(SCCHN)的多模态治疗通常涉及放射治疗和基于顺铂的治疗。DNA 修复机制(如核苷酸切除修复(NER)途径)的活性升高与顺铂和可能的 RT 抵抗有关,其中 ERCC1 是一个限速元件。我们已经确定了人乳头瘤病毒(HPV)阴性的 SCCHN 患者在接受手术[±辅助放疗/放化疗(CRT)]治疗后切除修复交叉互补组 1(ERCC1)的表达。
我们使用免疫荧光染色和自动定量分析(AQUA)用三种 ERCC1 抗体(8F1、FL297 和 HPA029773)评估了存档肿瘤中的 ERCC1 蛋白表达。使用分类和回归树(CART)方法分析确定了高/低 ERCC1 表达之间的截止点。多变量分析调整了年龄、T 和 N 期。Kaplan-Meier 曲线确定了中位生存期。比较了初始肿瘤和复发性疾病时的 ERCC1 表达。评估了抗体的性能特征。
根据 AQUA 分析,使用 8F1/2009、FL297 和 HPA029773 定义了 ERCC1 低/高组。在接受手术加辅助放疗/CRT 治疗的患者中,ERCC1 低组的中位生存期长于 ERCC1 高组(64 个月 vs. 29 个月;P=0.02;HPA029773)。仅接受手术治疗的患者中,使用 HPA029773 获得的数据表明生存无差异。复发性癌症的 ERCC1 AQUA 评分低于初始表现的肿瘤。广泛的特征分析表明,HPA029773 抗体具有最佳的特异性和性能。
使用 AQUA 和特定的 ERCC1 抗体 HPA029773,我们发现手术和辅助放疗治疗的患者中高/低 ERCC1 肿瘤的生存存在统计学差异。