Service of Obstetrics and Gynecology, Madrid, Spain.
Onco Targets Ther. 2013 Sep 16;9:1305-13. doi: 10.2147/OTT.S51532. eCollection 2013.
The aim of the study reported here was to assess the disease-free survival and overall survival of patients with endometrial cancer and to determine independent factors affecting the prognosis.
This was a retrospective study of a single-center clinical series of 276 patients (mean age 64 years) with histologically confirmed cancer of the corpus uteri. The standard treatments were extrafascial total hysterectomy and bilateral salpingo-oophorectomy with selective pelvic/para-aortic node dissection, according to risk for recurrence. Actuarial overall survival and disease-free survival were estimated according to the Kaplan-Meier method. Univariate and multivariate Cox proportional hazards analyses were used to assess the prognostic significance of the different variables.
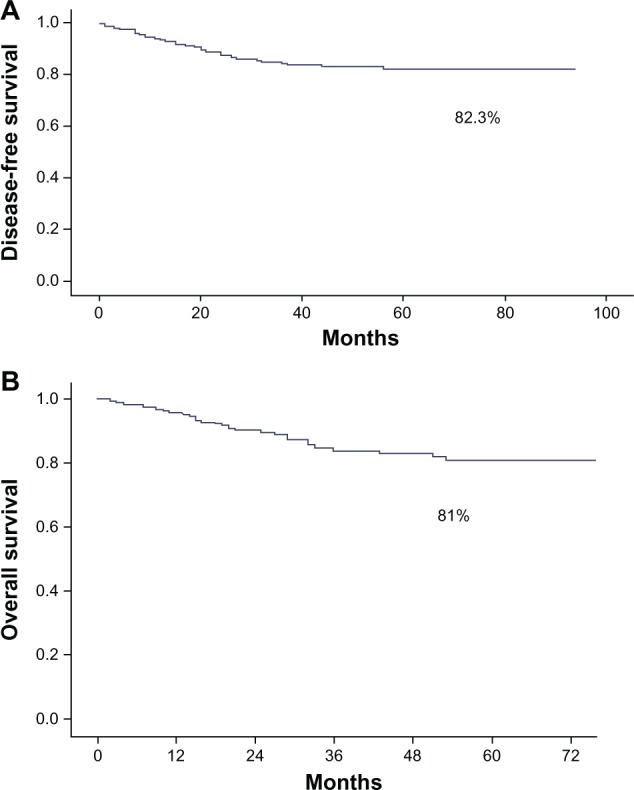
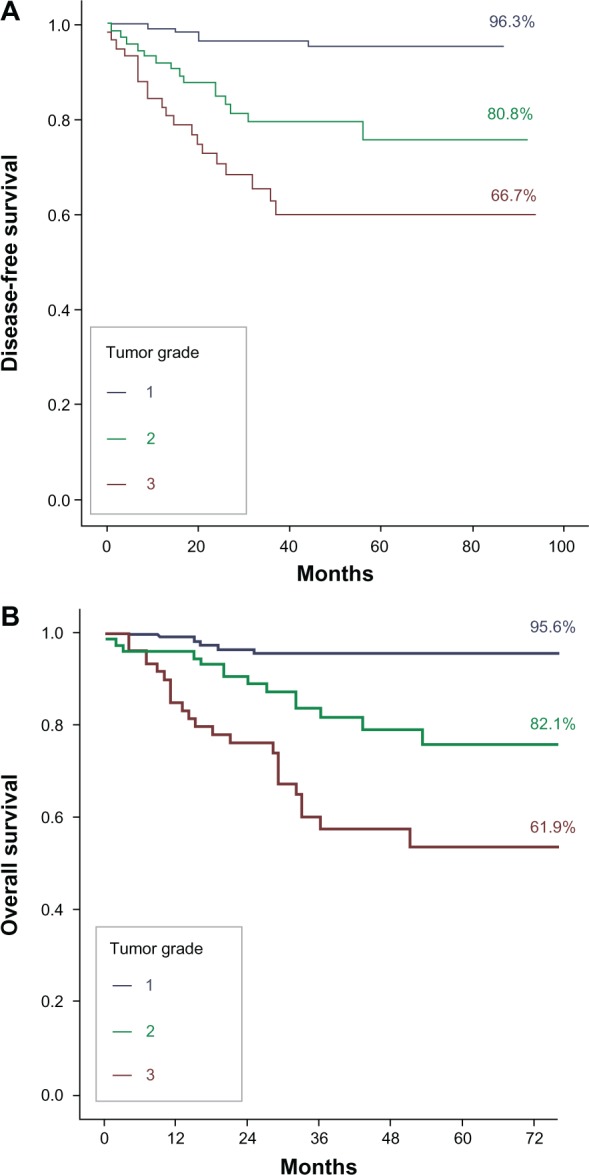
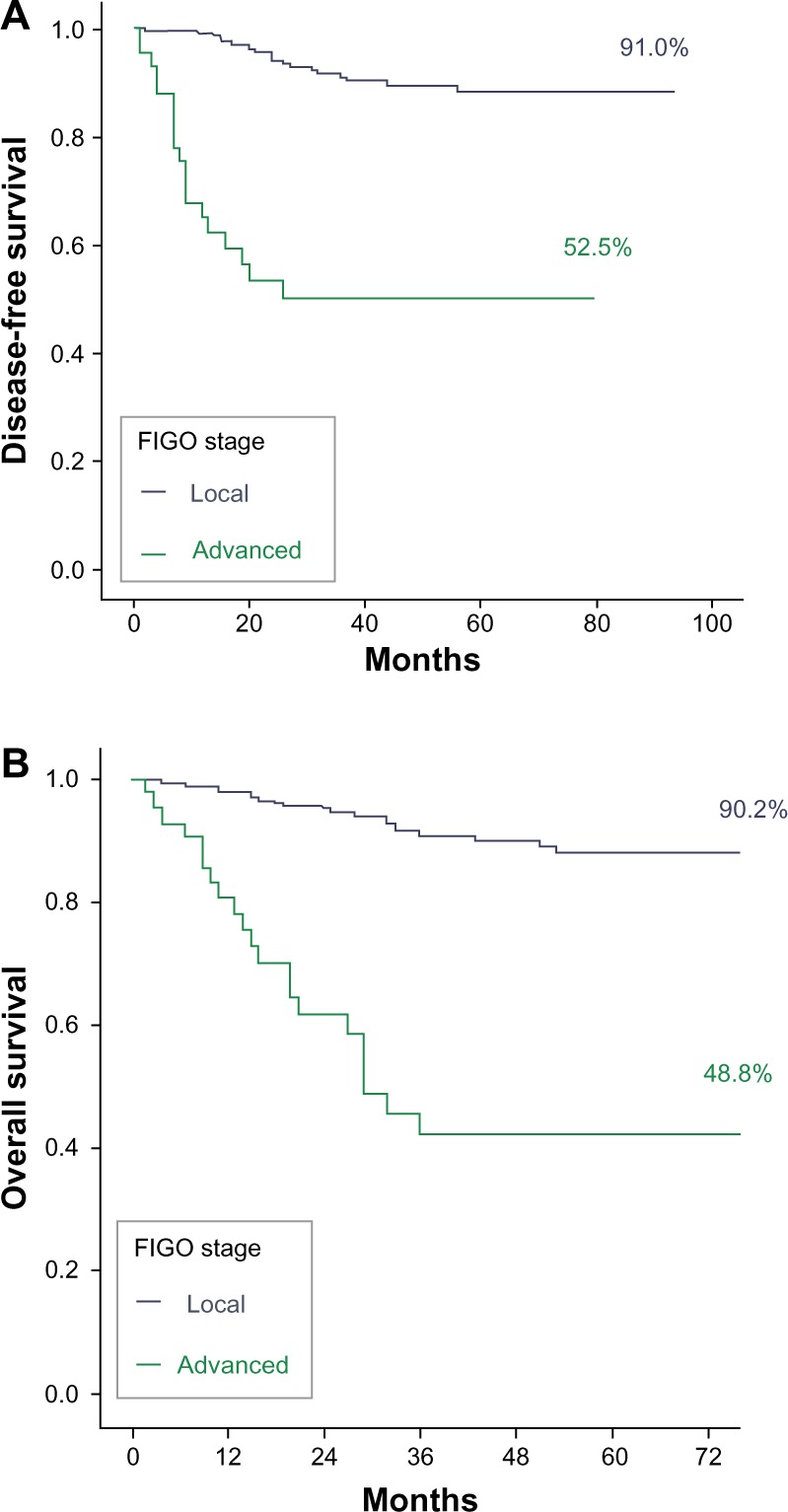
The estimated median follow-up, determined using the inverse Kaplan-Meier method, was 45 months (95% confidence interval [CI] 41.2-48.8) for disease-free survival and 46 months (95% CI 43.0-49.0) for overall survival. The statistically significant variables affecting disease-free survival and overall survival were age, serous-papillary and clear-cell histological types, outer-half myometrial invasion, advanced International Federation of Gynecology and Obstetrics (FIGO) stage, tumor grades G2 and G3, incomplete surgical resection, positive lymph nodes, lymphovascular space invasion, tumor remnants of >1 cm after surgery, and high-risk group. In the multivariate Cox regression model, predictors of tumor recurrence included advanced FIGO stage (hazard ratio [HR] 4.90, 95% CI 2.57-9.36, P < 0.001) and tumor grades G2 (HR 4.79, 95% CI 1.73-13.27, P = 0.003) and G3 (HR 7.56, 95% CI 2.75-20.73, P < 0.001). The same variables were also associated with a significantly higher risk of tumor-related mortality.
FIGO stage and tumor grade were independent prognostic factors of disease-free survival and overall survival in endometrial cancer patients. Outcome was also influenced by histopathologic type, myometrial and lymphovascular space invasion, lymph-node involvement, age, and tumor remnants after surgery, although a larger study sample is probably needed to demonstrate the independent association of these variables with survival.
本研究旨在评估子宫内膜癌患者的无病生存率和总生存率,并确定影响预后的独立因素。
这是一项回顾性单中心临床研究,纳入了 276 例(平均年龄 64 岁)经组织学证实的子宫体癌患者。根据复发风险,标准治疗为筋膜外全子宫切除术和双侧输卵管卵巢切除术,选择性盆腔/主动脉旁淋巴结清扫术。采用 Kaplan-Meier 法估计总生存率和无病生存率。采用单因素和多因素 Cox 比例风险分析评估不同变量的预后意义。
采用逆 Kaplan-Meier 法确定的中位随访时间,无病生存率为 45 个月(95%置信区间 [CI] 41.2-48.8),总生存率为 46 个月(95% CI 43.0-49.0)。影响无病生存率和总生存率的统计学显著变量为年龄、浆液性乳头状和透明细胞组织学类型、子宫肌层外 1/2 浸润、国际妇产科联合会(FIGO)晚期分期、肿瘤分级 G2 和 G3、手术不彻底、淋巴结阳性、脉管间隙浸润、术后肿瘤残留>1cm、高危组。在多因素 Cox 回归模型中,肿瘤复发的预测因素包括 FIGO 晚期分期(风险比 [HR] 4.90,95%CI 2.57-9.36,P<0.001)和肿瘤分级 G2(HR 4.79,95%CI 1.73-13.27,P=0.003)和 G3(HR 7.56,95%CI 2.75-20.73,P<0.001)。这些变量同样与肿瘤相关死亡率显著升高相关。
FIGO 分期和肿瘤分级是子宫内膜癌患者无病生存率和总生存率的独立预后因素。组织病理学类型、肌层和脉管间隙浸润、淋巴结受累、年龄以及术后肿瘤残留等因素也会影响预后,但可能需要更大的研究样本才能证明这些变量与生存的独立相关性。