Department of Medicine, Division of Infectious Diseases, Duke University Medical Center, Durham, North Carolina, United States of America ; Department of Medicine, Division of Infectious Diseases, Durham Veterans Affairs Medical Center, Durham, North Carolina, United States of America.
PLoS One. 2013 Oct 3;8(10):e76225. doi: 10.1371/journal.pone.0076225. eCollection 2013.
Gram-negative bacterial bloodstream infection (BSI) is a serious condition with estimated 30% mortality. Clinical outcomes for patients with severe infections improve when antibiotics are appropriately chosen and given early. The objective of this study was to estimate the association of prior healthcare exposure on time to appropriate antibiotic therapy in patients with gram-negative BSI.
We performed a multicenter cohort study of adult, hospitalized patients with gram-negative BSI using time to event analysis in nine community hospitals from 2003-2006. Event time was defined as the first administration of an antibiotic with in vitro activity against the infecting organism. Healthcare exposure status was categorized as community-acquired, healthcare-associated, or hospital-acquired. Time to appropriate therapy among groups of patients with differing healthcare exposure status was assessed using Kaplan-Meier analyses and multivariate Cox proportional hazards models.
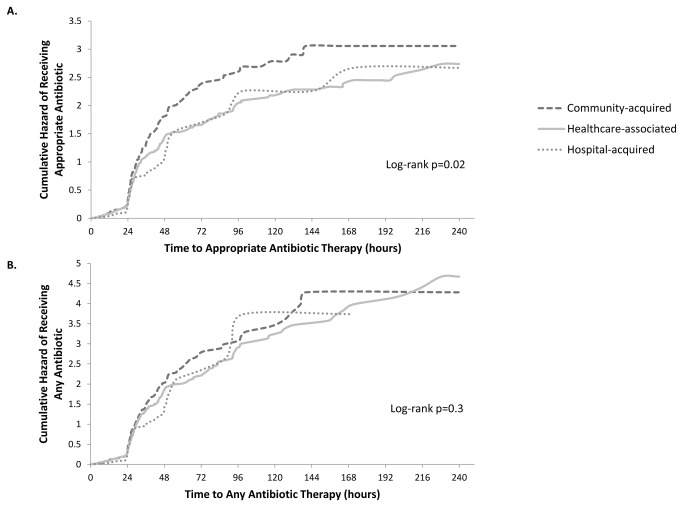
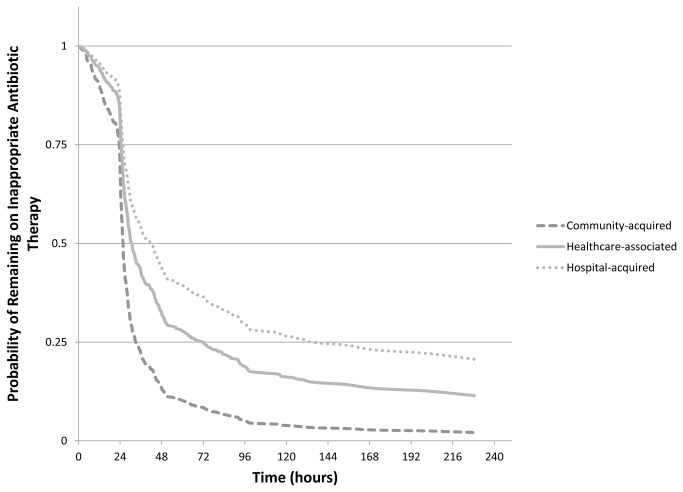
The cohort included 578 patients with gram-negative BSI, including 320 (55%) healthcare-associated, 217 (38%) community-acquired, and 41 (7%) hospital-acquired infections. 529 (92%) patients received an appropriate antibiotic during their hospitalization. Time to appropriate therapy was significantly different among the groups of healthcare exposure status (log-rank p=0.02). Time to first antibiotic administration regardless of drug appropriateness was not different between groups (p=0.3). The unadjusted hazard ratios (HR) (95% confidence interval) were 0.80 (0.65-0.98) for healthcare-associated and 0.72 (0.63-0.82) for hospital-acquired, relative to patients with community-acquired BSI. In multivariable analysis, interaction was found between the main effect and baseline Charlson comorbidity index. When Charlson index was 3, adjusted HRs were 0.66 (0.48-0.92) for healthcare-associated and 0.57 (0.44-0.75) for hospital-acquired, relative to patients with community-acquired infections.
Patients with healthcare-associated or hospital-acquired BSI experienced delays in receipt of appropriate antibiotics for gram-negative BSI compared to patients with community-acquired BSI. This difference was not due to delayed initiation of antibiotic therapy, but due to the inappropriate choice of antibiotic.
革兰氏阴性菌血流感染(BSI)是一种严重的疾病,死亡率估计为 30%。当抗生素选择得当并尽早使用时,重症感染患者的临床结局会得到改善。本研究旨在评估患者先前的医疗保健暴露对革兰氏阴性菌 BSI 患者接受适当抗生素治疗时间的影响。
我们对 2003 年至 2006 年期间在 9 家社区医院住院的革兰氏阴性菌 BSI 成年患者进行了一项多中心队列研究,采用事件时间分析。事件时间定义为首次给予具有体外抗感染菌活性的抗生素的时间。医疗保健暴露状况分为社区获得性、医疗保健相关性和医院获得性。使用 Kaplan-Meier 分析和多变量 Cox 比例风险模型评估具有不同医疗保健暴露状况的患者组之间的适当治疗时间。
该队列包括 578 例革兰氏阴性菌 BSI 患者,其中 320 例(55%)为医疗保健相关性、217 例(38%)为社区获得性、41 例(7%)为医院获得性感染。529 例(92%)患者在住院期间接受了适当的抗生素治疗。各组的医疗保健暴露状况的治疗时间明显不同(对数秩检验,p=0.02)。无论药物是否适当,首次抗生素给药时间在组间均无差异(p=0.3)。未调整的危险比(HR)(95%置信区间)分别为医疗保健相关性的 0.80(0.65-0.98)和医院获得性的 0.72(0.63-0.82),与社区获得性 BSI 患者相比。在多变量分析中,主要效应与基线 Charlson 合并症指数之间存在交互作用。当 Charlson 指数为 3 时,医疗保健相关性的调整 HR 为 0.66(0.48-0.92),医院获得性的调整 HR 为 0.57(0.44-0.75),与社区获得性感染患者相比。
与社区获得性 BSI 患者相比,医疗保健相关性或医院获得性 BSI 患者接受革兰氏阴性菌 BSI 适当抗生素治疗的时间延迟。这种差异不是由于抗生素治疗的延迟开始,而是由于抗生素的选择不当。