Stanford University (White), Stanford Prevention Research Center, Stanford, the University of California, Berkeley (Dow), School of Public Health, Berkeley, California.
Am J Prev Med. 2013 Nov;45(5):533-42. doi: 10.1016/j.amepre.2013.06.020.
Treatment for tobacco dependence is not available in many low-resource settings, especially in developing countries.
To test the impact of a novel mix of monetary and social incentives on smoking abstinence in rural communities of Thailand.
An RCT of commitment contracts and team incentives for rural smokers to quit smoking. Smokers were not blinded to treatment status, although the assessor of the biochemical urine test was.
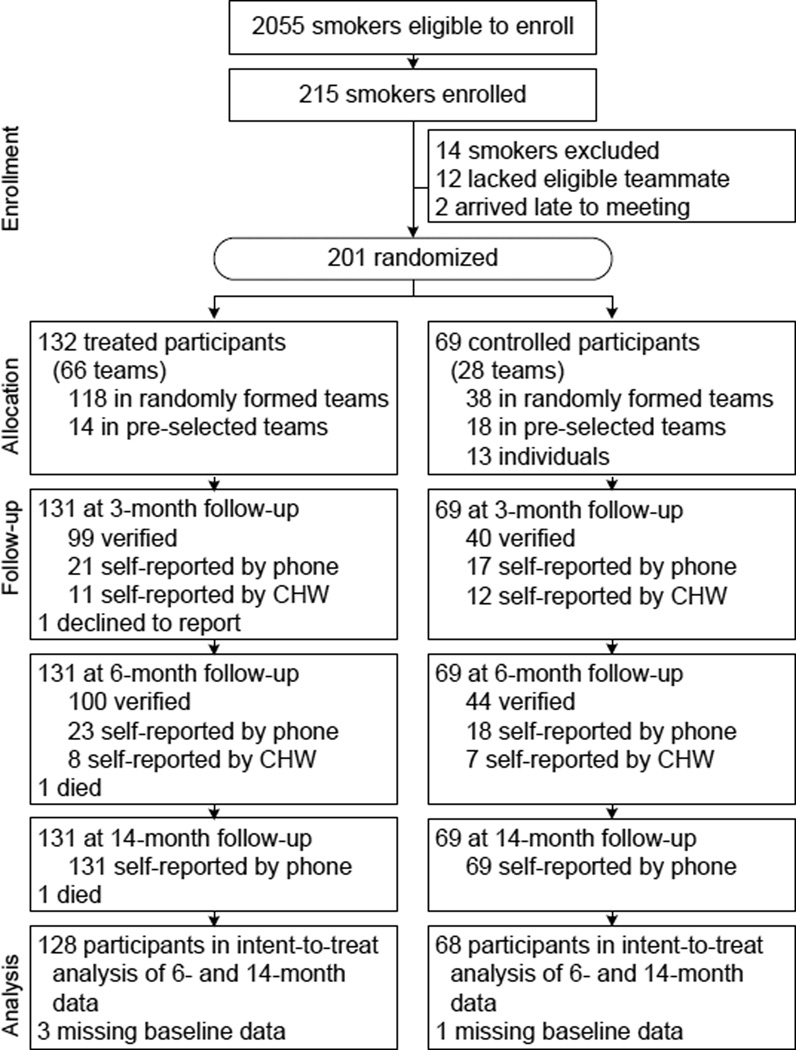
SETTING/PARTICIPANTS: All adult smokers living in the study area were eligible to participate; 215 adult smokers from 42 villages in Nakhon Nayok province, Thailand, participated. Fourteen smokers who lacked teammates were dropped.
A total of 201 smokers were assigned to a two-person team, and then randomly assigned by team (in a 2:1 ratio) with computer-generated random numbers to receive smoking-cessation counseling (control group) or counseling plus offer of a commitment contract, team incentives, and text message reminders for smoking cessation at 3 months (intervention group).
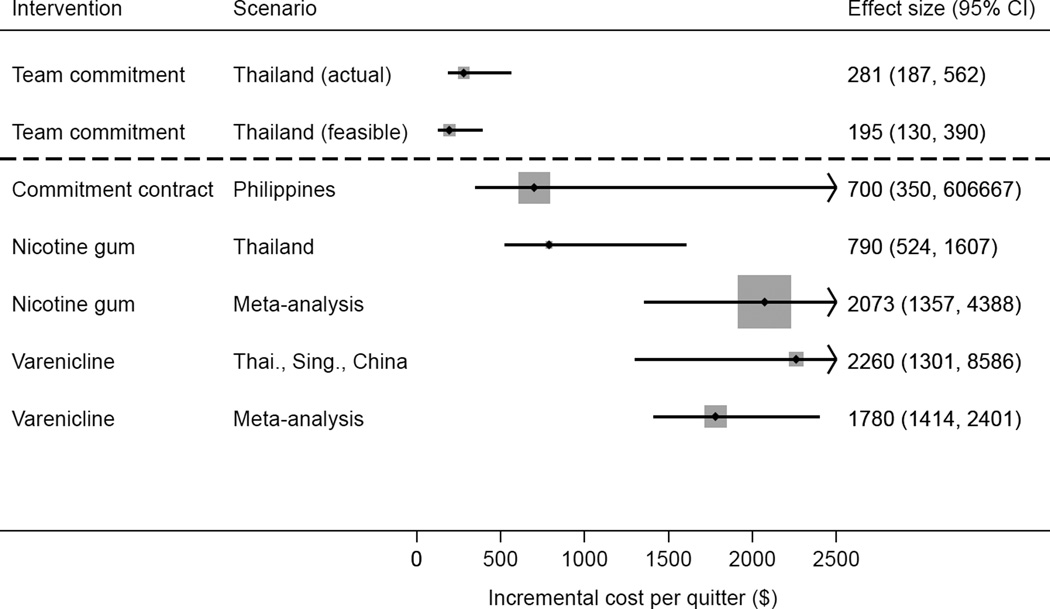
The primary outcome was biochemically verified 7-day abstinence at 6 months, assessed on an intention-to-treat basis. Secondary outcomes include study participation, biochemically verified abstinence at 3 months, self-reported abstinence at 14 months, and the incremental cost per quitter of the intervention, nicotine gum, and varenicline in Thailand. Data were collected in 2010-2011 and analyzed in 2012.
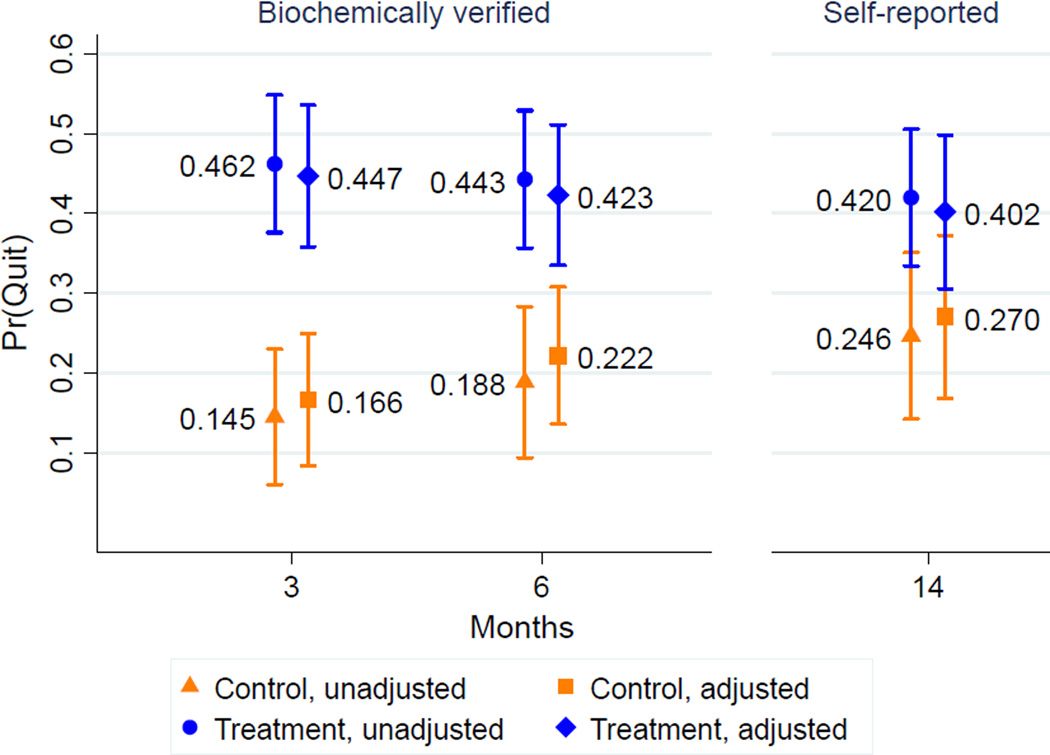
The trial enrolled 215 (10.5%) of 2055 smokers. The abstinence rate was 46.2% (61/132) in the intervention group and 14.5% (10/69) in the control group (adjusted OR 7.5 [3.0-18.6]) at 3 months; 44.3% (58/131) and 18.8% (13/69) at the primary end point of 6 months (adjusted OR 4.2 [1.8-9.7]); and 42.0% (55/131) and 24.6% (17/69) at 14 months (adjusted OR 2.2 [1.0-4.8]). The purchasing power parity-adjusted incremental cost per quitter from the intervention is $281 (95% CI=$187, $562), less than for nicotine gum ($1780, 95% CI=$1414, $2401) or varenicline ($2073, 95% CI=$1357, $4388) in Thailand.
The intervention enhanced abstinence by 91%-136% at 6 months, relative to the control group, although self-reports at 14 months suggest tapering of the treatment effect. The intervention may offer a viable, cost-effective alternative to current smoking-cessation approaches in low-resource settings.
This study is registered at ClinicalTrials.gov NCT01311115.
在许多资源匮乏的环境中,特别是在发展中国家,无法提供针对烟草依赖的治疗。
测试一种新的金钱和社会激励混合方案对泰国农村社区戒烟的影响。
农村吸烟者戒烟承诺合同和团队激励的 RCT。虽然生物化学尿液测试的评估者没有被蒙蔽,但吸烟者对治疗状况是知情的。
地点/参与者:居住在研究区域的所有成年吸烟者都有资格参加;215 名来自泰国那空那育府 42 个村庄的成年吸烟者参加了研究。由于缺乏队友,14 名吸烟者被排除在外。
共有 201 名吸烟者被分配到两人一组,然后通过计算机生成的随机数按团队(2:1 比例)随机分配,接受戒烟咨询(对照组)或咨询加承诺合同、团队激励和戒烟短信提醒,为期 3 个月(干预组)。
主要结局是基于意向治疗的 6 个月时生物化学验证的 7 天戒烟率。次要结局包括研究参与、3 个月时生物化学验证的戒烟率、14 个月时自我报告的戒烟率,以及泰国干预、尼古丁贴片和伐伦克林的每个戒烟者的增量成本。数据于 2010-2011 年收集,2012 年进行分析。
该试验共纳入了 215 名(2055 名吸烟者的 10.5%)吸烟者。3 个月时,干预组的戒烟率为 46.2%(61/132),对照组为 14.5%(10/69)(调整后的 OR 7.5 [3.0-18.6]);主要终点 6 个月时,干预组为 44.3%(58/131),对照组为 18.8%(13/69)(调整后的 OR 4.2 [1.8-9.7]);14 个月时,干预组为 42.0%(55/131),对照组为 24.6%(17/69)(调整后的 OR 2.2 [1.0-4.8])。从干预中获得的每个戒烟者的购买力平价调整增量成本为 281 美元(95%CI=187,562),低于泰国的尼古丁贴片(1780 美元,95%CI=1414,2401)或伐伦克林(2073 美元,95%CI=1357,4388)。
与对照组相比,该干预措施在 6 个月时将戒烟率提高了 91%-136%,尽管 14 个月时的自我报告显示治疗效果逐渐减弱。该干预措施可能为资源匮乏环境中的当前戒烟方法提供一种可行的、具有成本效益的替代方案。
本研究在 ClinicalTrials.gov 注册,编号为 NCT01311115。