Yoneda Hiroshi, Suzuki Michiyasu, Ishihara Hideyuki, Koizumi Hiroyasu, Nomura Sadahiro, Fujii Masami
Department of Neurosurgery, Clinical Neuroscience, Higher Biointegration, Yamaguchi University Graduate School of Medicine.
Neurol Med Chir (Tokyo). 2014;54(3):205-10. doi: 10.2176/nmc.cr2012-0343. Epub 2013 Oct 21.
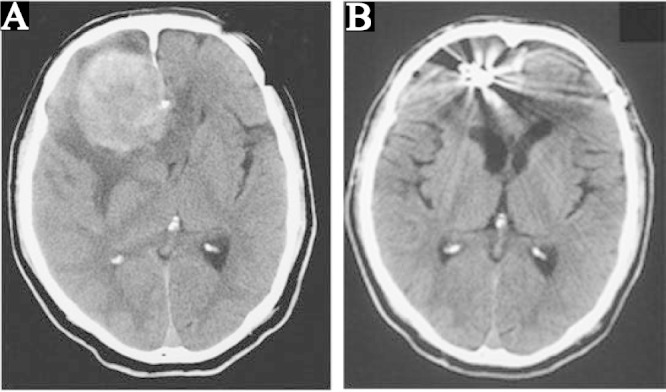
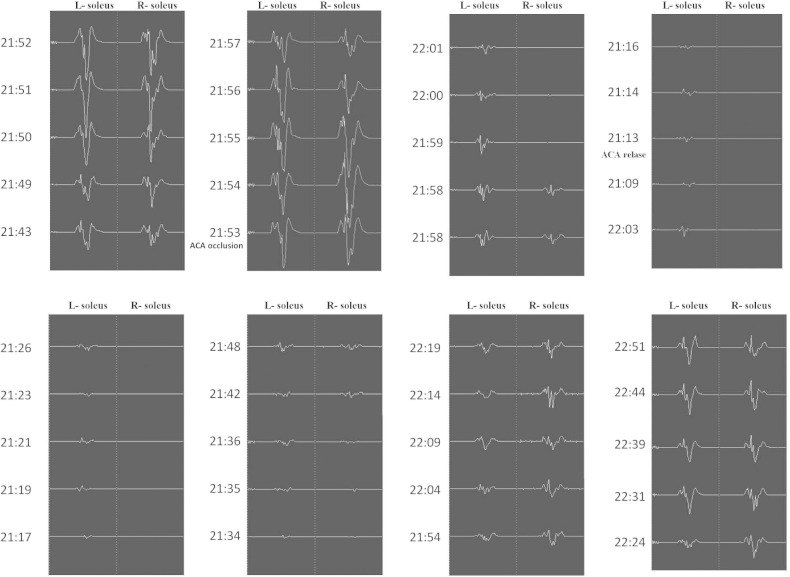
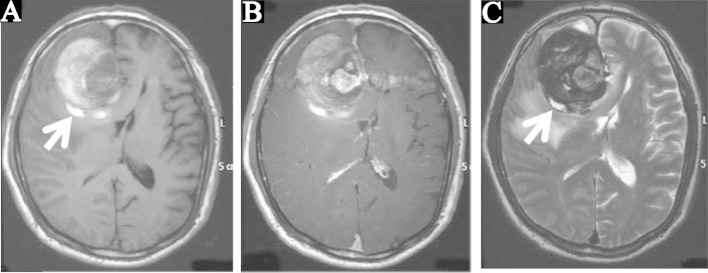
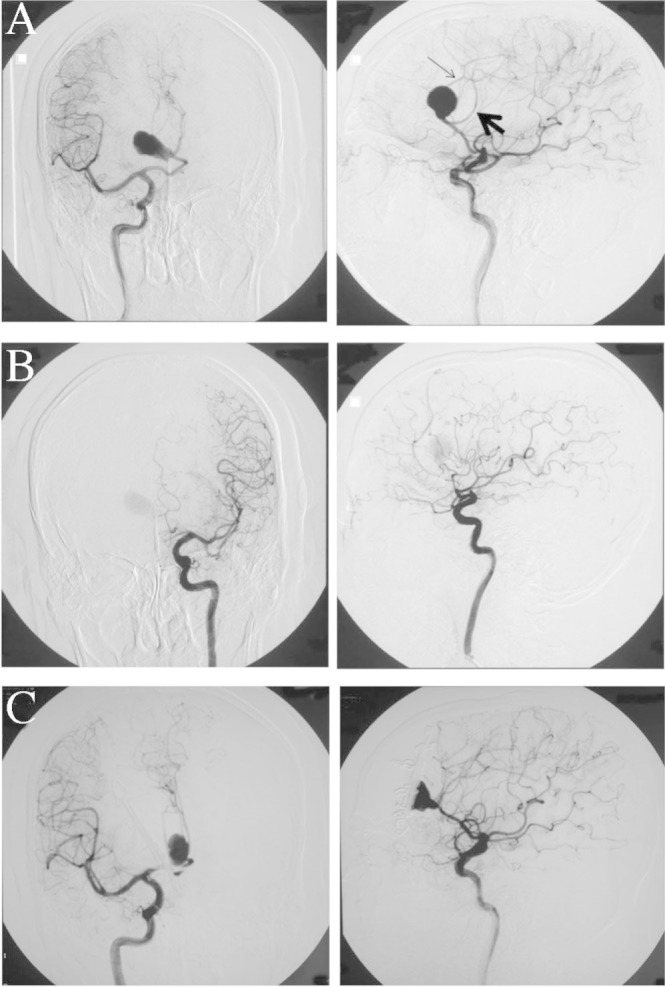
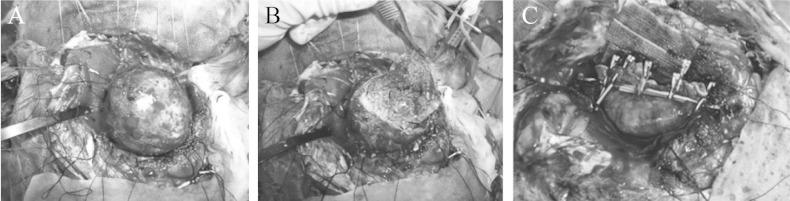
Giant aneurysms of the distal anterior cerebral artery (ACA), especially the azygos ACA, are rare. We treated a patient with giant aneurysm of the azygos ACA who underwent aspiration of thrombus and clipping under monitoring of motor evoked potentials of the lower extremities (L-MEPs), resulting in remarkable recovery of motor and intellectual function. A 72-year-old male was admitted with left motor weakness persisting for 2 weeks. Neurologically, disorientation and intellectual impairment were also noted. Imaging disclosed a 60-mm diameter aneurysm with heterochronous thrombi arising from the distal bifurcation of the azygos ACA. One month after the onset, radical surgery was scheduled. The azygos ACA was secured and the aneurysm was dissected, and the distal parts of the azygos ACA were confirmed. After removal of the thrombus, the neck was reconstructed with eight clips. L-MEPs disappeared due to occlusion of the azygos ACA for 20 minutes but reappeared after 22 minutes and normalized 78 minutes after reperfusion. Motor weakness improved entirely with mini-mental state examination score of 29 points at 1 month after surgery. One year later, Wechsler Adult Intelligence Scale-Third Edition and Wechsler Memory Scale-Revised scores reached normal levels. Review of reported cases found this aneurysm tends to occur in males in their 50s to 70s presenting with mass sign. Decompression of the aneurysm in the frontal lobe and monitoring of L-MEPs during temporary occlusion of the ACA are important.
大脑前动脉(ACA)远端的巨大动脉瘤,尤其是单干型ACA的巨大动脉瘤,较为罕见。我们治疗了一名患有单干型ACA巨大动脉瘤的患者,该患者在下肢运动诱发电位(L-MEPs)监测下进行了血栓抽吸和夹闭手术,术后运动和智力功能显著恢复。一名72岁男性因左侧运动无力持续2周入院。神经学检查还发现其存在定向障碍和智力损害。影像学检查显示,在单干型ACA远端分叉处有一个直径60毫米的动脉瘤,并伴有不同时期的血栓形成。发病1个月后,计划进行根治性手术。首先固定单干型ACA,然后解剖动脉瘤,并确认单干型ACA的远端部分。清除血栓后,用8个夹子重建瘤颈。单干型ACA闭塞20分钟时L-MEPs消失,但22分钟后重新出现,并在再灌注78分钟后恢复正常。术后1个月,运动无力完全改善,简易精神状态检查评分为29分。1年后,韦氏成人智力量表第三版和韦氏记忆量表修订版得分达到正常水平。回顾已报道的病例发现,这种动脉瘤倾向于发生在50至70岁的男性,表现为占位体征。额叶动脉瘤减压和ACA临时闭塞期间L-MEPs监测很重要。