Cancer Sciences Academic Unit and University of Southampton Clinical Trials Unit, Faculty of Medicine, University of Southampton and University Hospital Southampton Foundation Trust, Tremona Road, Southampton SO16 6YA, UK.
Centre for Statistics in Medicine, Wolfson College Annexe, Oxford OX2 6UD, UK.
Br J Cancer. 2014 Jan 7;110(1):230-41. doi: 10.1038/bjc.2013.650. Epub 2013 Oct 22.
Black ethnic groups have a higher breast cancer mortality than Whites. American studies have identified variations in tumour biology and unequal health-care access as causative factors. We compared tumour pathology, treatment and outcomes in three ethnic groups in young breast cancer patients treated in the United Kingdom.
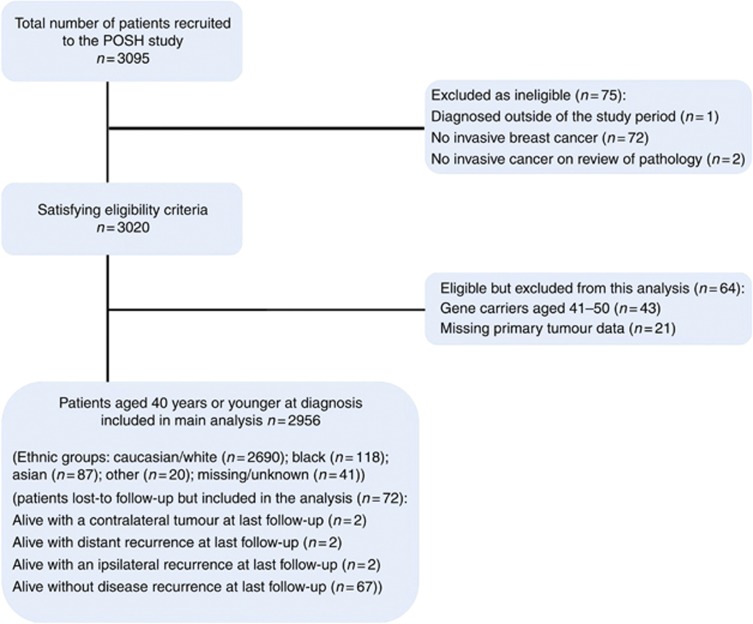
Women aged ≤ 40 years at breast cancer diagnosis were recruited to the POSH national cohort study (MREC: 00/06/69). Personal characteristics, tumour pathology and treatment data were collected at diagnosis. Follow-up data were collected annually. Overall survival (OS) and distant relapse-free survival (DRFS) were assessed using Kaplan-Meier curves, and multivariate analyses were performed using Cox regression.
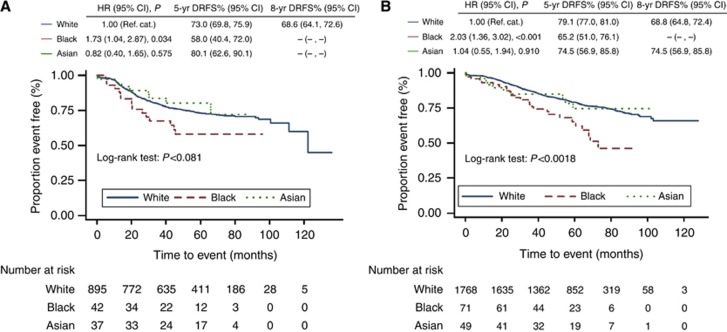
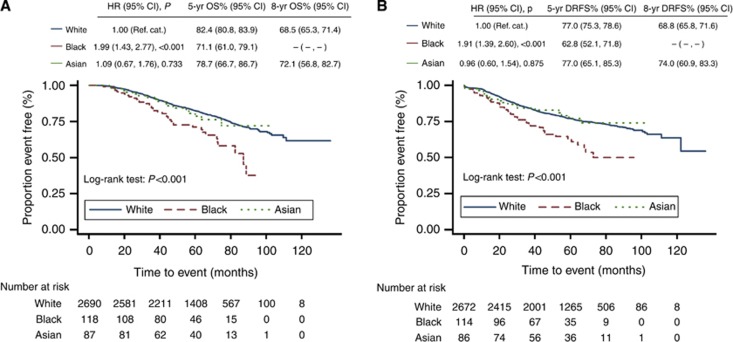
Ethnicity data were available for 2915 patients including 2690 (91.0%) Whites, 118 (4.0%) Blacks and 87 (2.9%) Asians. Median tumour diameter at presentation was greater in Blacks than Whites (26.0 mm vs 22.0 mm, P=0.0103), and multifocal tumours were more frequent in both Blacks (43.4%) and Asians (37.0%) than Whites (28.9%). ER/PR/HER2-negative tumours were significantly more frequent in Blacks (26.1%) than Whites (18.6%, P=0.043). Use of chemotherapy was similarly high in all ethnic groups (89% B vs 88.6% W vs 89.7% A). A 5-year DRFS was significantly lower in Blacks than Asians (62.8% B vs 77.0% A, P=0.0473) or Whites (62.8 B% vs 77.0% W, P=0.0053) and a 5-year OS for Black patients, 71.1% (95% CI: 61.0-79.1%), was significantly lower than that of Whites (82.4%, 95% CI: 80.8-83.9%, W vs B: P=0.0160). In multivariate analysis, Black ethnicity had an effect on DRFS in oestrogen receptor (ER)-positive patients that is independent of body mass index, tumour size, grade or nodal status, HR: 1.60 (95% CI: 1.03-2.47, P=0.035).
Despite equal access to health care, young Black women in the United Kingdom have a significantly poorer outcome than White patients. Black ethnicity is an independent risk factor for reduced DRFS particularly in ER-positive patients.
黑人族群的乳腺癌死亡率高于白人族群。美国的研究已经确定了肿瘤生物学的差异和医疗保健获取的不平等是造成这种情况的原因。我们比较了在英国接受治疗的年轻乳腺癌患者的三个族群的肿瘤病理学、治疗和结局。
在 POSH 全国队列研究(MREC:00/06/69)中招募了年龄在乳腺癌诊断时≤ 40 岁的女性。在诊断时收集了个人特征、肿瘤病理学和治疗数据。每年进行随访数据收集。使用 Kaplan-Meier 曲线评估总生存(OS)和远处无复发生存(DRFS),并使用 Cox 回归进行多变量分析。
共纳入 2915 例患者的种族数据,其中包括 2690 例(91.0%)白人、118 例(4.0%)黑人以及 87 例(2.9%)亚洲人。黑人患者的肿瘤直径中位数大于白人(26.0 毫米 vs 22.0 毫米,P=0.0103),而且黑人(43.4%)和亚洲人(37.0%)的多发病灶更为常见,而白人则为 28.9%。黑人患者中 ER/PR/HER2 阴性肿瘤的比例明显高于白人(26.1% vs 18.6%,P=0.043)。所有族群的化疗使用率均较高(黑人 89% vs 白人 88.6% vs 亚洲人 89.7%)。黑人患者的 5 年 DRFS 明显低于亚洲人(62.8% vs 77.0%,P=0.0473)或白人(62.8% vs 77.0%,P=0.0053),黑人患者的 5 年 OS 为 71.1%(95%CI:61.0-79.1%),明显低于白人(82.4%,95%CI:80.8-83.9%,W 与 B:P=0.0160)。多变量分析显示,黑人族群的种族对雌激素受体(ER)阳性患者的 DRFS 有影响,这独立于体重指数、肿瘤大小、分级或淋巴结状态,HR:1.60(95%CI:1.03-2.47,P=0.035)。
尽管获得了平等的医疗保健机会,但英国的年轻黑人女性的预后明显差于白人患者。黑人族群是降低 DRFS 的独立危险因素,尤其是在 ER 阳性患者中。