Authors' Affiliations: Departments of Thoracic/Head and Neck Medical Oncology, Biostatistics and Applied Mathematics, Translational Molecular Pathology, Diagnostic Imaging, Diagnostic Radiology, and Bioinformatics and Computational Biology; Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston; The Hamon Center for Therapeutic Oncology Research and Departments of Internal Medicine and Pharmacology, The University of Texas Southwestern Medical Center, Dallas, Texas; Solid Tumor Oncology and Investigational Therapeutics, Levine Cancer Institute, Charlotte, North Carolina; Medical Oncology, Yale Cancer Center, New Haven, Connecticut; Division of Medical Oncology, University of Ottawa, Ottawa, Ontario; Department of Oncology and Diagnostic Sciences, University of Maryland Dental School, Baltimore, Maryland; UC San Diego Moores Cancer Center, La Jolla, California; and Centre de Recherche en Cancérologie de Lyon, UMR INSERM 1052-CNRS 5286, Centre Léon Bérard, Lyon, France.
Clin Cancer Res. 2013 Dec 15;19(24):6967-75. doi: 10.1158/1078-0432.CCR-12-1818. Epub 2013 Oct 28.
To report the clinical efficacy of sorafenib and to evaluate biomarkers associated with sorafenib clinical benefit in the BATTLE (Biomarker-Integrated Approaches of Targeted Therapy for Lung Cancer Elimination) program.
Patients with previously treated non-small cell lung cancer (NSCLC) received sorafenib until progression or unacceptable toxicity. Eight-week disease control rate (DCR), progression-free survival (PFS), and overall survival (OS) were assessed. Prespecified biomarkers included K-RAS, EGFR, and B-RAF mutations, and EGFR gene copy number. Gene expression profiles from NSCLC cell lines and patient tumor biopsies with wild-type EGFR were used to develop a sorafenib sensitivity signature (SSS).
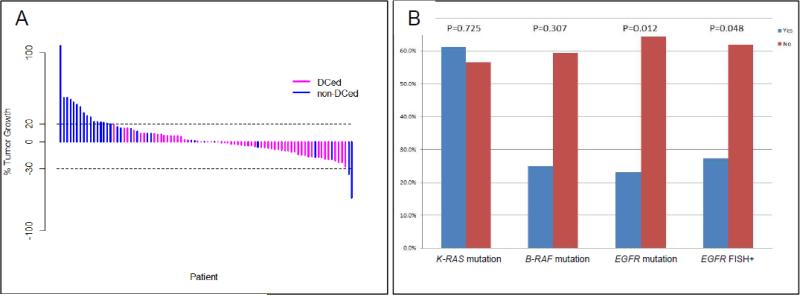
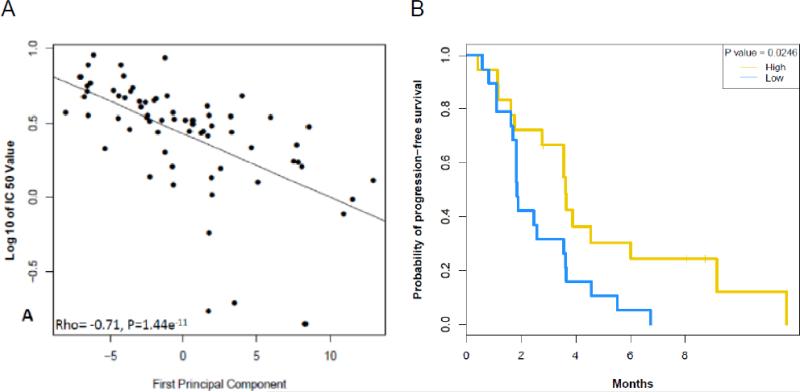
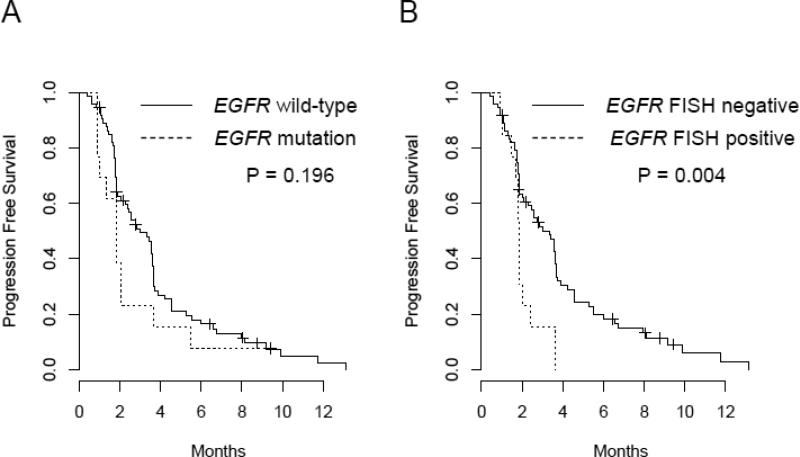
A total of 105 patients were eligible and randomized to receive sorafenib. Among 98 patients evaluable for eight-week DCR, the observed DCR was 58.2%. The median PFS and OS were 2.83 [95% confidence interval (CI), 2.04-3.58] and 8.48 months (95% CI, 5.78-10.97), respectively. Eight-week DCR was higher in patients with wild-type EGFR than patients with EGFR mutation (P = 0.012), and in patients with EGFR gene copy number gain (FISH-positive) versus patients FISH-negative (P = 0.048). In wild-type EGFR tumors, the SSS was associated with improved PFS (median PFS 3.61 months in high SSS vs. 1.84 months in low SSS; P = 0.026) but not with eight-week DCR. Increased expression of fibroblast growth factor-1, NF-κB, and hypoxia pathways were identified potential drivers of sorafenib resistance.
Sorafenib demonstrates clinical activity in NSCLC, especially with wild-type EGFR. SSS was associated with improved PFS. These data identify subgroups that may derive clinical benefit from sorafenib and merit investigation in future trials.
报告索拉非尼的临床疗效,并评估与索拉非尼临床获益相关的生物标志物,这是在 BATTLE(生物标志物综合方法靶向治疗肺癌消除)计划中进行的。
先前治疗过的非小细胞肺癌(NSCLC)患者接受索拉非尼治疗,直至疾病进展或出现不可接受的毒性。评估 8 周的疾病控制率(DCR)、无进展生存期(PFS)和总生存期(OS)。预设的生物标志物包括 K-RAS、EGFR 和 B-RAF 突变以及 EGFR 基因拷贝数。利用 NSCLC 细胞系和野生型 EGFR 的患者肿瘤活检标本的基因表达谱,开发了一种索拉非尼敏感性特征(SSS)。
共有 105 名符合条件的患者被随机分配接受索拉非尼治疗。在 98 名可评估 8 周 DCR 的患者中,观察到的 DCR 为 58.2%。中位 PFS 和 OS 分别为 2.83 个月(95%置信区间 [CI],2.04-3.58)和 8.48 个月(95%CI,5.78-10.97)。与 EGFR 突变患者相比,野生型 EGFR 患者的 8 周 DCR 更高(P = 0.012),与 EGFR 基因拷贝数增加(FISH 阳性)患者相比,FISH 阴性患者的 8 周 DCR 更高(P = 0.048)。在野生型 EGFR 肿瘤中,SSS 与改善的 PFS 相关(高 SSS 组的中位 PFS 为 3.61 个月,低 SSS 组为 1.84 个月;P = 0.026),但与 8 周 DCR 无关。鉴定出成纤维细胞生长因子-1、NF-κB 和缺氧途径的高表达是索拉非尼耐药的潜在驱动因素。
索拉非尼在 NSCLC 中显示出临床活性,尤其是在野生型 EGFR 患者中。SSS 与改善的 PFS 相关。这些数据确定了可能从索拉非尼中获得临床获益的亚组,值得在未来的试验中进一步研究。