1The Pulmonary Center, Boston University School of Medicine, Boston, MA. 2Division of Pulmonary, Allergy, and Critical Care Medicine Internal Medicine, Boston Medical Center, Boston, MA. 3Department of Medicine, Boston Medical Center, Boston, MA. 4Center for Healthcare Organization & Implementation Research, Edith Nourse Rogers Memorial VA Hospital, Bedford, MA. 5The Dartmouth Institute for Health Policy and Clinical Practice, Dartmouth Medical School, Hanover, NH.
Crit Care Med. 2014 Mar;42(3):625-31. doi: 10.1097/CCM.0000000000000026.
Trends in severe sepsis mortality derived from administrative data may be biased by changing International Classification of Diseases, 9th Revision, Clinical Modification, coding practices. We sought to determine temporal trends in severe sepsis mortality using clinical trial data that does not rely on International Classification of Diseases, 9th Revision, Clinical Modifications coding and compare mortality trends in trial data with those observed from administrative data.
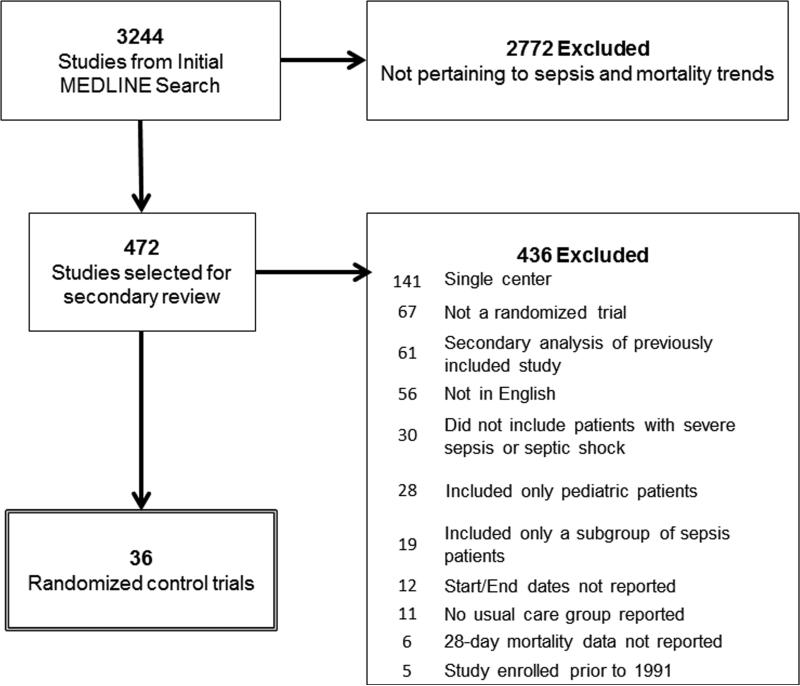
We searched MEDLINE for multicenter randomized trials that enrolled patients with severe sepsis from 1991 to 2009. We calculated standardized mortality ratios for each trial from observed 28-day mortality of usual care participants and predicted mortality from severity-of-illness scores. To compare mortality trends from clinical trials to administrative data, we identified adult severe sepsis hospitalizations in the Nationwide Inpatient Sample, 1993-2009, using two previously validated algorithms.
In-patient.
Patients with severe sepsis or septic shock.
None.
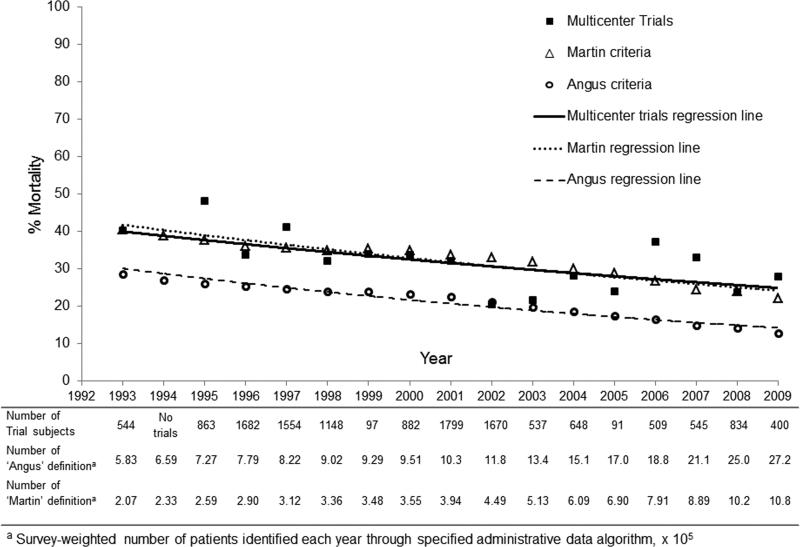
Of 3,244 potentially eligible articles, we included 36 multicenter severe sepsis trials, with a total of 14,418 participants in a usual care arm. Participants with severe sepsis receiving usual care had a 28-day mortality of 33.2%. Observed mortality decreased 3.0% annually (95% CI, 0.8%-5.0%; p = 0.009), decreasing from 46.9% (standardized mortality ratio 0.94; 95% CI, 0.86-1.03) during years 1991-1995 to 29% (standardized mortality ratio 0.53; 95% CI, 0.50-0.57) during years 2006-2009 (3.0% annual change). Trends in hospital mortality among patients with severe sepsis identified from administrative data (Angus definition, 4.7% annual change; 95% CI, 4.1%-5.3%; p = 0.69 and Martin definition, 3.5% annual change; 95% CI, 3.0%-4.1%; p = 0.97) were similar to trends identified from clinical trials.
Since 1991, patients with severe sepsis enrolled in usual care arms of multicenter randomized trials have experienced decreasing mortality. The mortality trends identified in clinical trial participants appear similar to those identified using administrative data and support the use of administrative data to monitor mortality trends in patients with severe sepsis.
源于行政数据的严重脓毒症死亡率趋势可能受到国际疾病分类第 9 版临床修订版(ICD-9-CM)编码实践改变的影响。我们旨在使用不依赖 ICD-9-CM 编码的临床试验数据来确定严重脓毒症死亡率的时间趋势,并比较临床试验死亡率趋势与从行政数据中观察到的死亡率趋势。
我们在 MEDLINE 上搜索了 1991 年至 2009 年间多中心随机试验,这些试验招募了严重脓毒症患者。我们根据常规治疗组观察到的 28 天死亡率和严重程度评分预测死亡率,计算了每个试验的标准化死亡率比。为了比较临床试验和行政数据的死亡率趋势,我们使用了两个先前验证过的算法,从 1993 年至 2009 年全国住院患者样本中确定了成人严重脓毒症住院患者。
住院患者。
患有严重脓毒症或脓毒性休克的患者。
无。
在 3244 篇潜在合格的文章中,我们纳入了 36 项多中心严重脓毒症试验,共有 14418 名常规治疗组患者参与。接受常规治疗的严重脓毒症患者 28 天死亡率为 33.2%。观察到的死亡率每年下降 3.0%(95%CI,0.8%-5.0%;p = 0.009),从 1991 年至 1995 年的 46.9%(标准化死亡率比 0.94;95%CI,0.86-1.03)降至 2006 年至 2009 年的 29%(标准化死亡率比 0.53;95%CI,0.50-0.57)(每年 3.0%的变化)。从行政数据中确定的严重脓毒症患者的住院死亡率趋势(安格斯定义,每年 4.7%的变化;95%CI,4.1%-5.3%;p = 0.69 和马丁定义,每年 3.5%的变化;95%CI,3.0%-4.1%;p = 0.97)与临床试验中确定的趋势相似。
自 1991 年以来,参加多中心随机试验常规治疗组的严重脓毒症患者死亡率呈下降趋势。临床试验参与者确定的死亡率趋势与使用行政数据确定的死亡率趋势相似,支持使用行政数据监测严重脓毒症患者的死亡率趋势。