From the University of Groningen, Groningen, the Netherlands (D.Z., H.J.L.H.); Showa University School of Medicine, Tokyo (T.A.); Reata Pharmaceuticals, Irving, TX (P.A., M.C., A.G., M.K., C.J.M.); University of Chicago (G.L.B.) and AbbVie Pharmaceuticals (M.H.) - both in Chicago; Statistics Collaborative, Washington, DC (H.C.-S., J.W., D.W.); University of Glasgow, Glasgow, United Kingdom (J.J.M.); Rigshospitalet, University of Copenhagen, Copenhagen (H.-H.P.); Istituto di Ricovero e Cura a Carattere Scientifico-Istituto di Ricerche Farmacologiche Mario Negri, Bergamo, Italy (G.R.); University of Texas Southwestern Medical Center, Dallas (R.D.T.); University of California, Irvine (N.D.V.); University of Würzburg, Würzburg, Germany (C.W.); and Stanford University, Palo Alto, CA (G.M.C.).
N Engl J Med. 2013 Dec 26;369(26):2492-503. doi: 10.1056/NEJMoa1306033. Epub 2013 Nov 9.
Although inhibitors of the renin-angiotensin-aldosterone system can slow the progression of diabetic kidney disease, the residual risk is high. Whether nuclear 1 factor (erythroid-derived 2)-related factor 2 activators further reduce this risk is unknown.
We randomly assigned 2185 patients with type 2 diabetes mellitus and stage 4 chronic kidney disease (estimated glomerular filtration rate [GFR], 15 to <30 ml per minute per 1.73 m(2) of body-surface area) to bardoxolone methyl, at a daily dose of 20 mg, or placebo. The primary composite outcome was end-stage renal disease (ESRD) or death from cardiovascular causes.
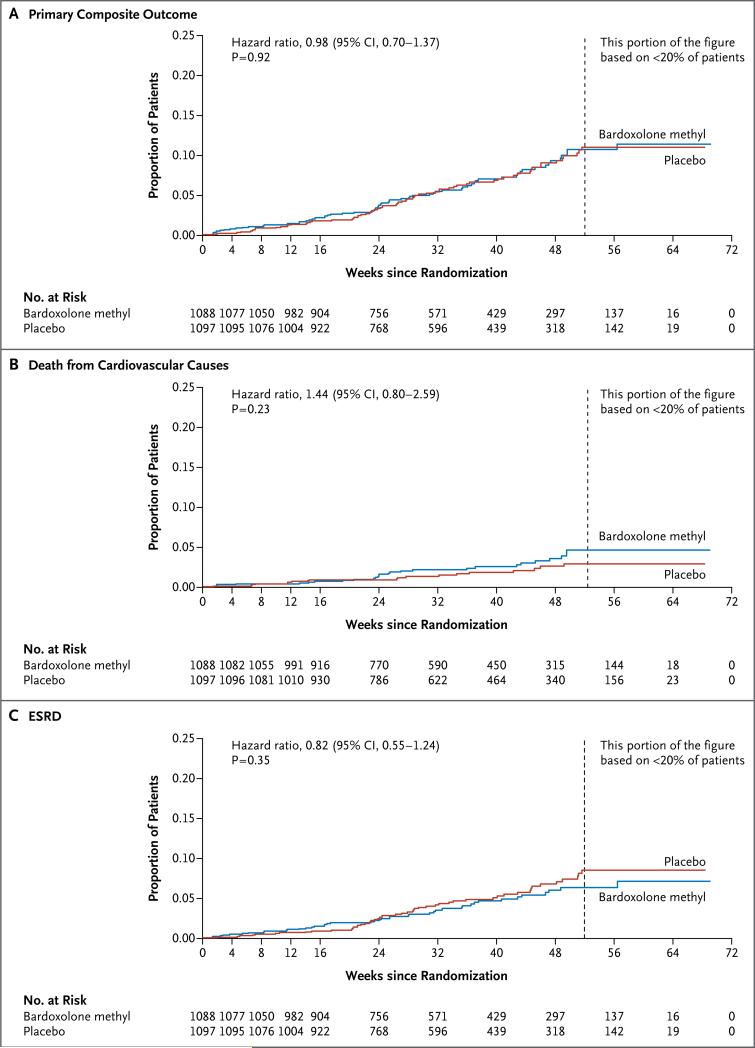
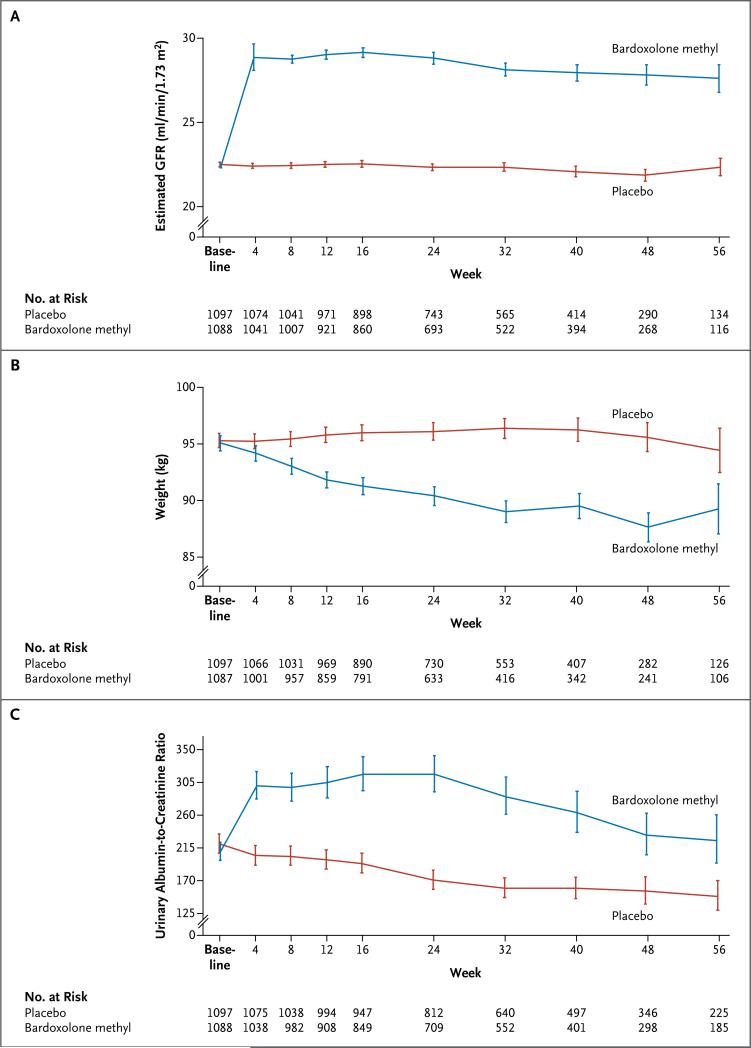
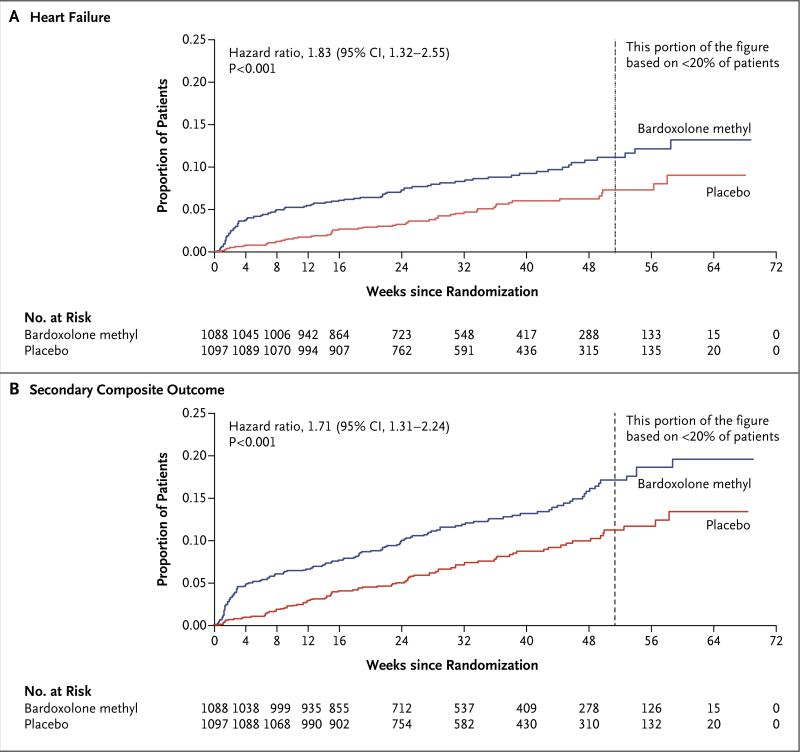
The sponsor and the steering committee terminated the trial on the recommendation of the independent data and safety monitoring committee; the median follow-up was 9 months. A total of 69 of 1088 patients (6%) randomly assigned to bardoxolone methyl and 69 of 1097 (6%) randomly assigned to placebo had a primary composite outcome (hazard ratio in the bardoxolone methyl group vs. the placebo group, 0.98; 95% confidence interval [CI], 0.70 to 1.37; P=0.92). In the bardoxolone methyl group, ESRD developed in 43 patients, and 27 patients died from cardiovascular causes; in the placebo group, ESRD developed in 51 patients, and 19 patients died from cardiovascular causes. A total of 96 patients in the bardoxolone methyl group were hospitalized for heart failure or died from heart failure, as compared with 55 in the placebo group (hazard ratio, 1.83; 95% CI, 1.32 to 2.55; P<0.001). Estimated GFR, blood pressure, and the urinary albumin-to-creatinine ratio increased significantly and body weight decreased significantly in the bardoxolone methyl group, as compared with the placebo group.
Among patients with type 2 diabetes mellitus and stage 4 chronic kidney disease, bardoxolone methyl did not reduce the risk of ESRD or death from cardiovascular causes. A higher rate of cardiovascular events with bardoxolone methyl than with placebo prompted termination of the trial. (Funded by Reata Pharmaceuticals; BEACON ClinicalTrials.gov number, NCT01351675.).
尽管肾素-血管紧张素-醛固酮系统抑制剂可以减缓糖尿病肾病的进展,但仍存在较高的残余风险。核因子(红细胞衍生 2)相关因子 2 激活剂是否能进一步降低这种风险尚不清楚。
我们将 2185 例 2 型糖尿病和 4 期慢性肾脏病(估计肾小球滤过率[GFR]为 15 至<30 ml/min/1.73 m2 体表面积)患者随机分为两组,每日分别给予 bardoxolone 甲基 20 mg 或安慰剂。主要复合终点为终末期肾病(ESRD)或心血管原因死亡。
赞助商和指导委员会根据独立数据和安全监测委员会的建议终止了试验;中位随访时间为 9 个月。共有 1088 例随机分配至 bardoxolone 甲基组的患者中有 69 例(6%)和 1097 例随机分配至安慰剂组的患者中有 69 例(6%)发生主要复合终点(bardoxolone 甲基组与安慰剂组的危险比为 0.98;95%置信区间[CI]为 0.70 至 1.37;P=0.92)。在 bardoxolone 甲基组中,有 43 例患者发生 ESRD,27 例患者死于心血管原因;在安慰剂组中,有 51 例患者发生 ESRD,19 例患者死于心血管原因。bardoxolone 甲基组共有 96 例患者因心力衰竭住院或心力衰竭死亡,而安慰剂组为 55 例(危险比为 1.83;95%CI 为 1.32 至 2.55;P<0.001)。与安慰剂组相比,bardoxolone 甲基组的估计肾小球滤过率、血压和尿白蛋白与肌酐比值显著升高,体重显著下降。
在 2 型糖尿病和 4 期慢性肾脏病患者中,bardoxolone 甲基并不能降低 ESRD 或心血管原因死亡的风险。bardoxolone 甲基组心血管事件发生率高于安慰剂组,促使试验提前终止。(由 Reata 制药公司资助;BEACON 临床试验.gov 编号,NCT01351675)。