Casadio Valentina, Molinari Chiara, Calistri Daniele, Tebaldi Michela, Gunelli Roberta, Serra Luigi, Falcini Fabio, Zingaretti Chiara, Silvestrini Rosella, Amadori Dino, Zoli Wainer
Biosciences Laboratory, Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST) IRCCS, Via P, Maroncelli 40, Meldola 47014, Italy.
J Exp Clin Cancer Res. 2013 Nov 19;32(1):94. doi: 10.1186/1756-9966-32-94.
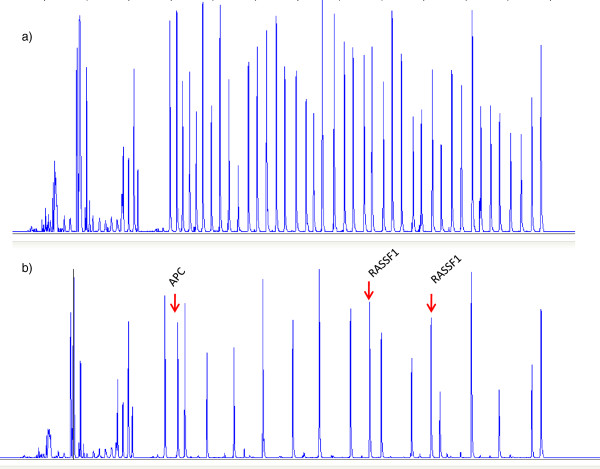
Although non muscle invasive bladder cancer (NMIBC) generally has a good long-term prognosis, up to 80% of patients will nevertheless experience local recurrence after the primary tumor resection. The search for markers capable of accurately identifying patients at high risk of recurrence is ongoing. We retrospectively evaluated the methylation status of a panel of 24 tumor suppressor genes (TIMP3, APC, CDKN2A, MLH1, ATM, RARB, CDKN2B, HIC1, CHFR, BRCA1, CASP8, CDKN1B, PTEN, BRCA2, CD44, RASSF1, DAPK1, FHIT, VHL, ESR1, TP73, IGSF4, GSTP1 and CDH13) in primary lesions to obtain information about their role in predicting local recurrence in NMIBC.
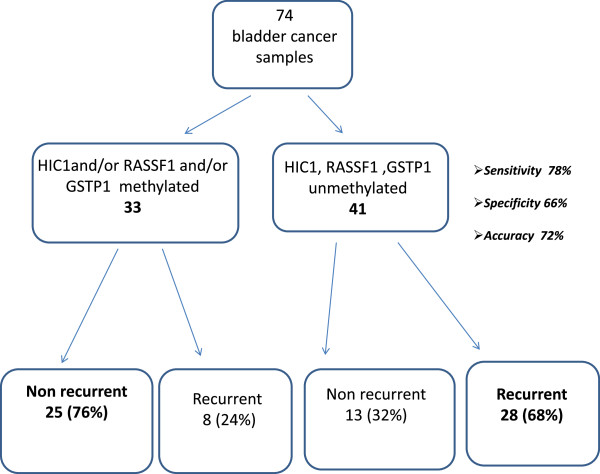
Formaldehyde-fixed paraffin-embedded (FFPE) samples from 74 patients operated on for bladder cancer were analyzed by methylation-specific multiplex ligation-dependent probe amplification (MS-MLPA): 36 patients had relapsed and 38 were disease-free at the 5-year follow up. Methylation status was considered as a dichotomous variable and genes showing methylation ≥20% were defined as "positive".
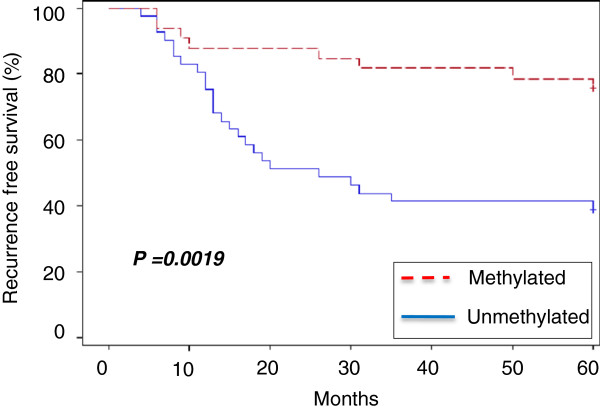
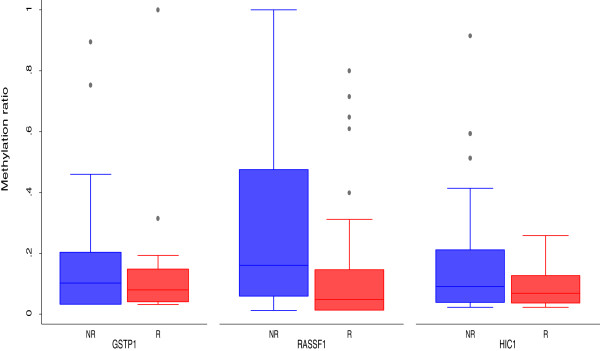
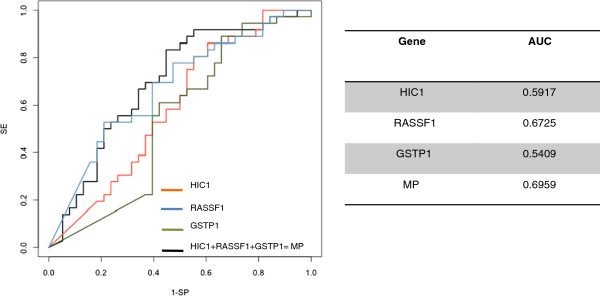
Methylation frequencies were higher in non recurring than recurring tumors. A statistically significant difference was observed for HIC1 (P = 0.03), GSTP1 (P = 0.02) and RASSF1 (P = 0.03). The combination of the three genes showed 78% sensitivity and 66% specificity in identifying recurrent patients, with an overall accuracy of 72%.
Our preliminary data suggest a potential role of HIC1, GSTP1 and RASSF1 in predicting local recurrence in NMIBC. Such information could help clinicians to identify patients at high risk of recurrence who require close monitoring during follow up.
尽管非肌层浸润性膀胱癌(NMIBC)通常具有良好的长期预后,但高达80%的患者在原发性肿瘤切除后仍会出现局部复发。寻找能够准确识别复发高危患者的标志物的工作正在进行中。我们回顾性评估了一组24个肿瘤抑制基因(TIMP3、APC、CDKN2A、MLH1、ATM、RARB、CDKN2B、HIC1、CHFR、BRCA1、CASP8、CDKN1B、PTEN、BRCA2、CD44、RASSF1、DAPK1、FHIT、VHL、ESR1、TP73、IGSF4、GSTP1和CDH13)在原发性病变中的甲基化状态,以获取它们在预测NMIBC局部复发中的作用的信息。
通过甲基化特异性多重连接依赖探针扩增(MS-MLPA)分析了74例接受膀胱癌手术患者的甲醛固定石蜡包埋(FFPE)样本:36例患者复发,38例在5年随访时无疾病复发。甲基化状态被视为二分变量,甲基化≥20%的基因被定义为“阳性”。
非复发性肿瘤的甲基化频率高于复发性肿瘤。观察到HIC1(P = 0.03)、GSTP1(P = 0.02)和RASSF1(P = 0.03)存在统计学显著差异。这三个基因的组合在识别复发患者方面显示出78%的敏感性和66%的特异性,总体准确率为72%。
我们的初步数据表明HIC1、GSTP1和RASSF1在预测NMIBC局部复发中具有潜在作用。这些信息可以帮助临床医生识别复发高危患者,以便在随访期间进行密切监测。